The present study investigated the sonographic characteristics of thyroid nodules with halos. The findings show that benign nodules were mainly characterized by a thin and uniform halo with good integrity, while malignant nodules had a thicker halo with uneven and irregular margins. The halos of benign nodules were mostly hyper- or iso-enhanced, whereas the halos of malignant nodules were predominantly hypo-enhanced. The AUC for CEUS, FNA, and CEUS + FNA were 0.751 (95% CI = 0.642–0.841), 0.863 (95% CI = 0.767–0.929), and 0.918 (95% CI = 0.834–0.967), respectively. The primary pathological components of the halo around malignant nodules were reactive hyperplastic fibrous tissue, and cervical lymph node metastasis occurred in only 13 malignant nodes with halos.
Thyroid cancer is receiving increasing attention as the incidence of thyroid cancer is gradually increasing. Ultrasound is used as an important tool for routine screening of thyroid disease. With the standardization of ultrasonography, an expert consensus has been formed on the ultrasonographic manifestations of thyroid cancer. However, in recent years, the acoustic halo of thyroid nodules has attracted much attention [9].
Halo refers to the hypoechoic zone around thyroid nodules. To date, there is still disagreement regarding the halo around thyroid nodules in helping to diagnose the nature of thyroid nodules [10,11,12,13,14]. Propper et al. reported that halos can occur around benign and malignant nodules, and may be a nonspecific sign of thyroid nodules [15]. The main reason for its formation is still unclear. A reasonable explanation is that, owing to the pathological tissue transition layer between the tumor and normal thyroid tissue, with the continuous growth of the tumor, the transition layer is continuously compressed, and the acoustic impedance value around the tumor is gradually transitioned. When the adjacent acoustic impedance difference in the transition layer is very small, the reflected and scattered signals of the ultrasonic wave are very small, and the phenomenon of a hypoechoic halo appears [16]. Clark et al. believed that the acoustic halo is caused by the vessels surrounding the adenoma [17, 18].
At present, few studies have elaborated on the traditional ultrasound and CEUS features of the halo, and studies summarizing the pathological features of the halo and predicting the risk of metastasis of malignant thyroid nodules are even rarer. Zhang [19] et al. found that the halo of malignant nodules is thicker and more irregular than that of benign nodules. In this study, we found that benign and malignant nodules have different halo appearances. The periphery of benign nodules is mainly composed of thin and uniform halos, with good integrity. The mean thickness of the benign nodule halo was approximately 0.75 ± 0.31 mm, which is consistent with the research results of Zhang [19]. The sensitivity and specificity were highest when the cutoff value was 1.09 mm, with 76.08% and 84.29%, respectively. This is because most thyroid adenomas have a complete fibrous capsule, resulting in blood vessels circulating under the capsule to form a thin and uniform halo. However, it was also found in this study that among the 50 benign nodules with halos, there were still 8 cases with irregular halos, accounting for approximately 16%. The reason for these conditions is that nodular goiter and follicular hyperplasia are proliferative disorders, and because the nodules are in different stages, hyperplasia squeezes the surrounding thyroid tissue, leading to pathological factors such as heterogeneity and atrophy of the halo. There is often extruded thyroid follicular tissue within the halo, and nodular goiter changes outside the halo rather than just compression of the atrophied thyroid gland, so the separation from the surrounding thyroid tissue is not clear [20], which manifests as an incomplete or irregular halo. This may also be one of the reasons why some nodular goiters are difficult to distinguish from thyroid cancer. Excitingly, in this study, it was found that the halos of malignant thyroid nodules were thicker and unevenly distributed in thickness, with a mean thickness of approximately 1.48 ± 0.51 mm, which was significantly thicker than that of benign nodules at 0.75 ± 0.31 mm (P < 0.05). The sensitivity and specificity of the diagnosis of malignant nodules were highest when the cutoff value was taken as 1.09 mm, with 85.45% and 80%, respectively. This is due to the aggressive growth of malignant tissues and the uneven distribution of neovascularization during tumor growth causing the nodules to grow in different directions. In the area with abundant neovascularization, the tissue grows faster and exerts more pressure on the surrounding tissues, and the inflammatory response is heavier, resulting in a thicker halo. In contrast, in areas with less neovascularization, the tumor grows relatively slowly, presses less on the surrounding tissue, and has a mild inflammatory response, so the halo is thinner and even disappears.
CEUS is a pure blood pool imaging technology that can dynamically observe the hemodynamic changes in thyroid nodules and their halos in real time. Although the value of CEUS is not confirmed in the TIRADS guidelines, it is generally accepted that CEUS has a positive role in the diagnosis of thyroid nodules [21,22,23,24]. In the present study, we further investigated the CEUS characteristics of halos. The halo of both benign and malignant nodules was predominantly hypo-enhanced, but 20% of benign nodules still showed ring enhancement. Based on this, 20 benign cases and 41 malignant cases were correctly diagnosed by CEUS in this study, and the sensitivity, specificity, accuracy, positive predictive value and negative predictive value of CEUS for diagnosing malignant thyroid lesions were 83.7%, 64.5%, 76.3%, 78.9% and 71.4%, respectively. The significant ring of hyper-enhancement of benign nodules especially thyroid adenomas, is because most benign nodules have a capsule with blood vessels distributed along the sub-capsule. For other types of benign nodules, the enhancement of the halo was almost synchronized with the nodule, which is attributed to the fact that benign nodules have a thin halo with blood vessels evenly distributed within and without compression. In addition, the “partial volume effect” also affects the enhancement of the thin halo, causing synchronous enhancement with the surrounding thyroid tissue, which provides a basis for the diagnosis of benign thyroid nodules [25]. In contrast to benign nodules, the flow in the halo of malignant nodules is mainly dotted distributed, which contributed to the fact that 98.1% of malignant nodules were hypo-enhanced on CEUS in this study. This is mainly due to changes such as edema, mucinous degeneration, inflammation, and fibrosis around the nodules, resulting in a decrease and compression of the vascular component in the halo.
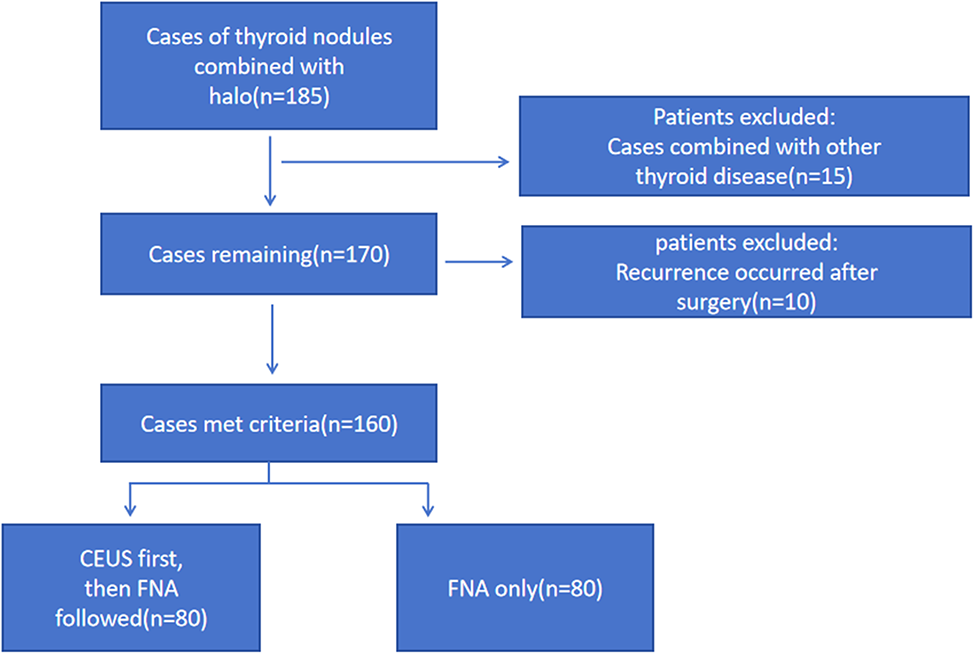
Ultrasound-guided FNA cytology has become the most direct method for diagnosing the nature of thyroid nodules because it is safe, accurate, rapid, and cost-effective, but it is still influenced by the operator and the satisfaction with the material obtained, and there were even discordant FNAC reports were distributed, which in turn required a repeat of the FNAC [26,27,28]. TH Yin [29] et al. reported that high-risk factors such as cystic nodules, nodules with hemorrhage and suspicious degenerating nodules may reduce specimen acquisition during FNA because viable tissue is rarely present in cystic nodules or it is difficult to distinguish between viable and inactive tissue with conventional ultrasound. In the present study, FNA diagnosed 20 benign and 50 malignant cases correctly, and the sensitivity, specificity, accuracy, positive predictive value and negative predictive value of FNA in diagnosing malignant thyroid lesions were 86.2%, 90.9%, 82.5%, 96.2% and 71.4%, respectively, higher than the results of CEUS, but still lower than the results of CEUS combined with FNA, which were 94.2%, 89.3%,92.5%, 94.2% and 89.3%, respectively. This is because the operator is unable to determine the distribution of the active component of the nodule during the process of FNA; although multidirectional and multiangle punctures can improve the effectiveness of extraction, there is still some uncertainty. However, with the assistance of CEUS, the operator can effectively avoid necrotic areas without vascular distribution and perform focused puncture on suspicious areas, to improve the efficiency and accuracy of the FNA results. The AUC of CEUS, FNA and CEUS combined with FNA were 75.1%, 86.3%, and 91.8%, respectively, further confirming that the combined method can effectively improve the diagnostic efficacy of nodules, which is consistent with the findings of TH Yin [29].
Although most thyroid cancers especially papillary carcinoma generally have slow disease progression with low mortality rates and a favorable long-term prognosis, the presence of cervical lymph node metastasis remains a significant risk factor for both local recurrence and distant metastasis [30,31,32,33]. Metastasis refers to the continued growth of tumor cells from the primary site to other sites through lymphatic vessels and blood vessels [34]. However, if the tumor is restrained or compressed by external force during growth, the expansive growth of the tumor will be inhibited, and the blood vessels or lymphatic vessels around the tumor will be blocked due to compression, which can theoretically inhibit the metastasis of tumor cells to a certain extent. In this study we summarized the pathology of the halo of benign and malignant nodules, and found that the main component of the halo of malignant nodules is fibrous connective tissue, which is caused by malignant tumors oppressing the surrounding tissues during the growth process and repeated inflammation. As the fibrous component of the acoustic corona increases, the vascular and lymphatic components further decrease, which reduces the possibility of tumor cell metastasis through lymphatic vessels. In addition, the increase in fiber content will also cause compression and squeezing on the lymphatic vessels, blocking the metastasis of tumor cells through the lymphatic vessels. Zheng et al. revealed that the pathological annulus fibrosus in the nonhyperechoic halo group often appeared incomplete, uneven, thin, or absent, and had a high rate of metastasis [35]. In fact, in the present study, only 13 out of 110 (11.5%) patients with malignant tumors had cervical lymph node metastases, and the findings are consistent with the literature. Analysis of the causes revealed that the halo of all 13 nodules was uneven in thickness, with the thinnest being only 3.4 mm, and their pathology suggested weak fibrous tissue, which may be an important cause of metastasis. Therefore, it is reasonable to speculate that malignant thyroid nodes with halos are less likely to have cervical lymph node metastasis than malignant nodes without halos. We will also increase the number of cases in the follow-up study to further test this speculation.
In summary, in the present study we found that malignant thyroid nodules had thicker and heterogeneous acoustic halos with poor integrity. The halo of malignant nodules was predominantly without or with little blood flow and showed hypo-enhancement on CEUS. The diagnostic efficacy of CEUS combined with FNA was significantly higher than that of CEUS. The pathological features of the halo were infiltrative inflammatory cells and a large amount of reactive hyperplastic fibrous tissue. In addition, we predicted a reduced risk of lymph node metastasis in malignant nodes with halos.
The present study has some limitations. Due to the limited number of cases, a larger sample is needed to verify the reliability of the findings of this study. In addition, because ultrasound is an examination that is greatly influenced by a variety of objective factors and subjective judgments, the measurement of the acoustic halo is influenced by many factors, such as instrument clarity, operating technique, scanning cross-section, and clinical experience. Therefore, it is necessary to improve the reproducibility and double-blindness of the study to obtain more reliable results.







留言 (0)