
記住我

This 66-year-old male presented with C3-C6 myelomalacia and spastic tetraparesis previously treated with decompressive laminectomy two years before. The onset of symptoms dated one year earlier with motor impairment and sensory deficit with caudal distribution and subsequent involvement of the upper limbs. He reported burning and crampy pain in the upper and lower limbs with tingling and pinpricking sensation in the extremities, tactile allodynia and paresthesia. Painful symptomatology was accompanied by continuous debilitating spasticity. He described a continuous sensation of stiffness, spasms, and involuntary contractions with difficulty in movement and either he was able to walk short distances with the aid of a walker or forced on a wheelchair. Neurological examination revealed modest motor autonomy on the bed, increased muscle tone, and need for assistance in all postural steps. Good trunk control in a sitting position without support. Standing and walking were possible with double support for very short stretches with a sharp gait and wide base, Mingazzini position with all 4 limbs without however being able to maintain it with a prevalence of deficit on the left.
High-dose steroid treatment did not modify the neurological deficits and induced iatrogenic diabetes. Electromyography (EMG) and Motor Evoked Potentials (MEPs) showed suffering of the central motor pathway on both upper and lower limbs. Painful symptomatology was refractory to neuropathic pain medications (pregabalin 150 mgx2/die and amitriptyline 32 mg/die) while buprenorphine was suspended due to allergic reactions. To manage pain, we decided to treat the patient with 10 kHz SCS.
An initial assessment was performed to ensure that there were no clinical exclusion criteria for the SCS implant procedure, and MRI exam confirmed outcomes of C3-C6 laminectomy, and the cervical spinal cord showed extensive intramedullary hyperintense T2 signal at that level (Fig. 1). The leads could not be implanted in the cervical epidural space due to presence of fibrotic scar tissue in the area of previous laminectomy. Therefore, decision was made to implant leads epidurally only along T8 to T11 (midT9-top T8) (Fig. 2). The patient underwent temporary 10 kHz SCS trial stimulation for 3 weeks with percutaneous leads; after reporting pain relief at lower limbs > 50% using the Visual Analogue Scale (VAS), he underwent permanent SCS device implant (Nevro Senza® Omnia™, Nevro Corp., Redwood City, CA, USA), which included the 2 percutaneous leads placed epidurally connected to an implantable pulse generator (IPG) in the lower back. Stimulation parameters included 10-kHz frequency, 30-µs pulse width delivered via bipole, and amplitude range of 0.5 to 3.5 mA. Optimal bipole location and amplitude were adjusted per patient feedback, as previously described [3,4,5].
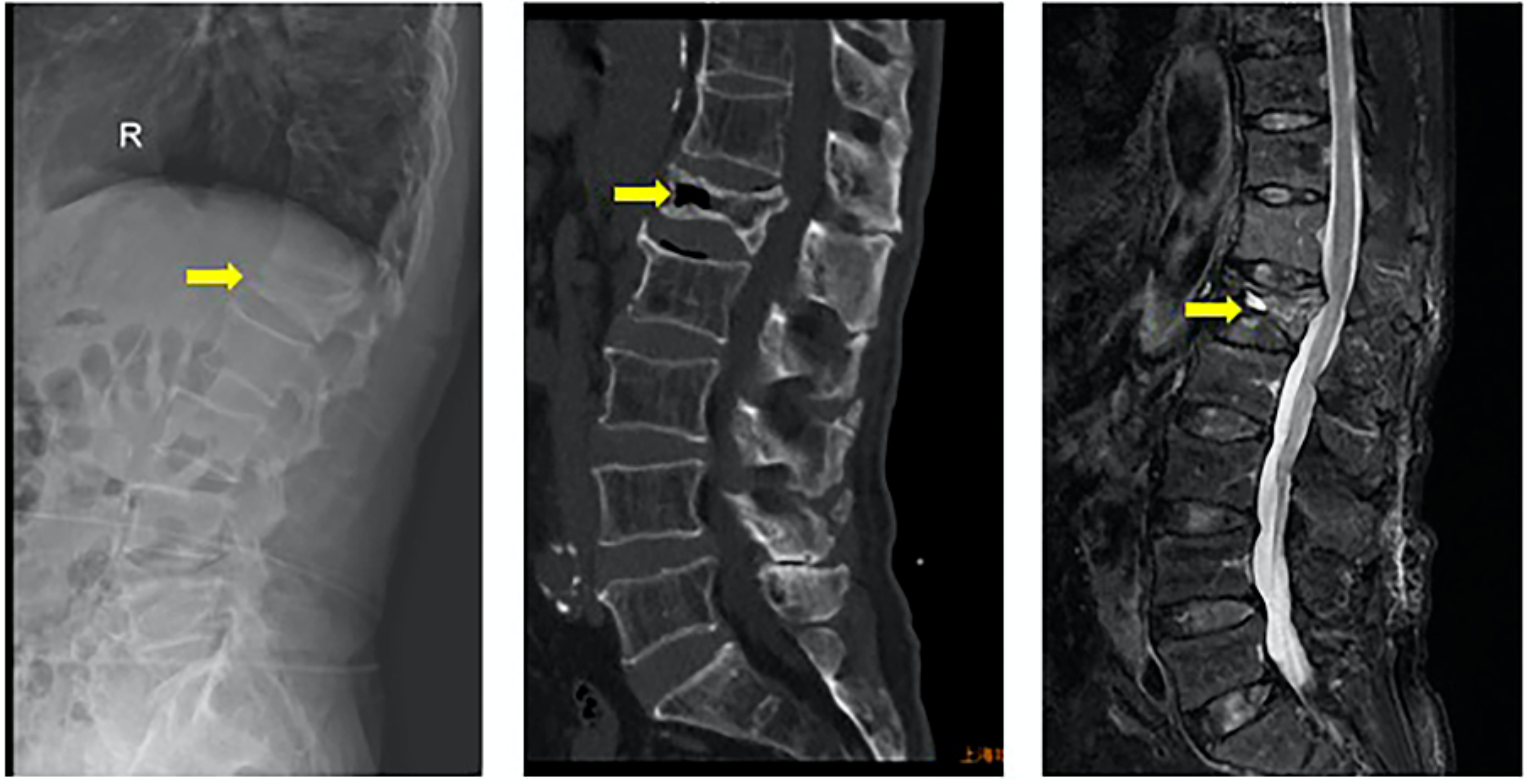
Fig. 1
Sagittal T2 MR Image showing abnormal intramedullary hyperintense signal at the level of cervical laminectomy
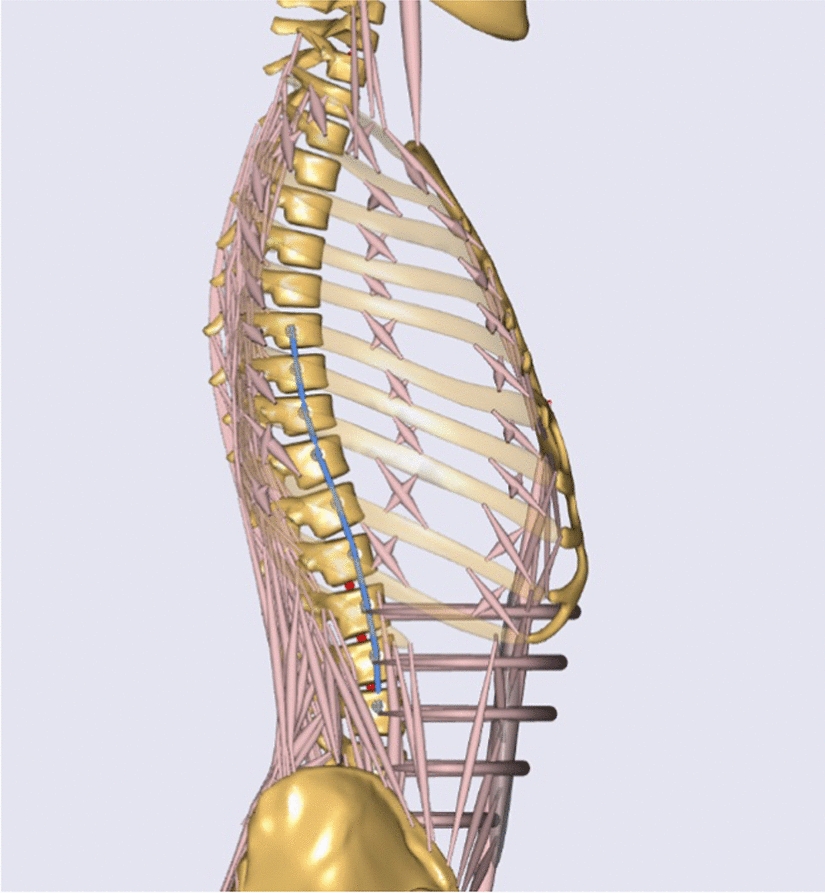
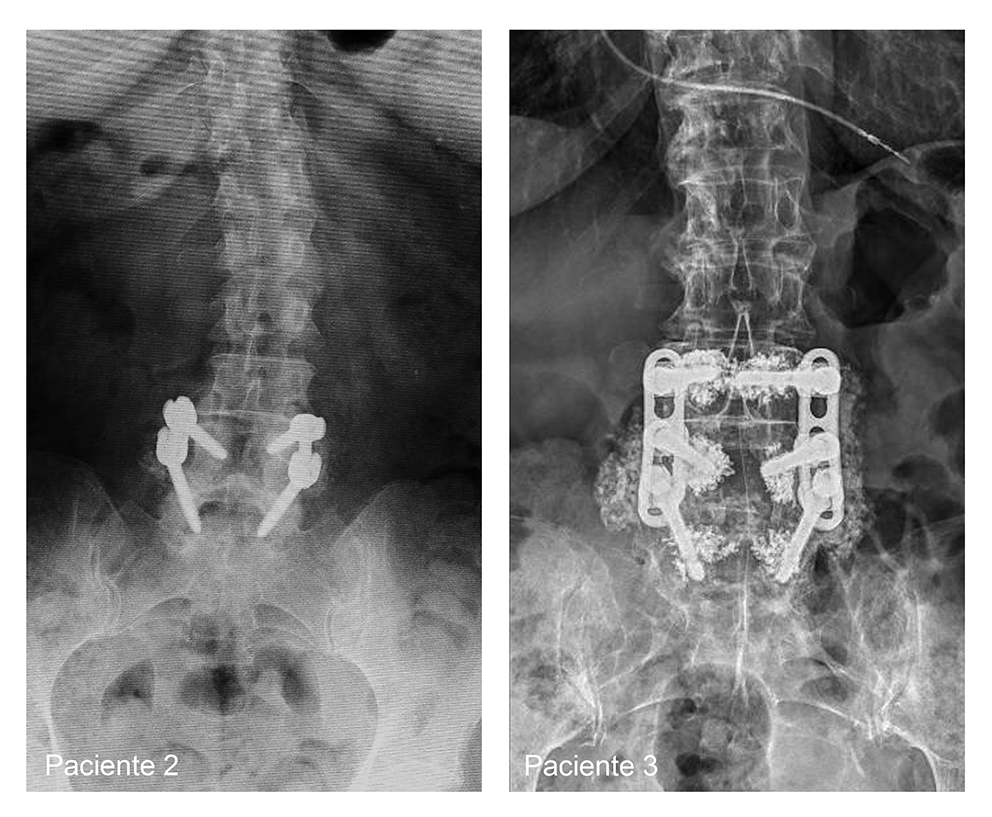
Fig. 2
X-ray image of two 8-contact percutaneous leads placed in the T8-T11 level
The immediate postoperative period was favorable and since trialing phase up to the last follow-up at 15 months the patient referred complete pain relief on the Visual Analogue Scale (VAS) at lower limbs, while upper limbs’ pain was stable; accordingly the Douleur Neuropathique en 4 Questionnaire (DN4) score changed from 7 at baseline (a score consistent with clinically confirmed neuropathic etiology of pain) to 0 at follow-up visits (Fig. 3). At admission the subject was in a severe disability category with a Oswestry Disability Index (ODI) score of 50% and a drastic improvement was observed in the disability level as the ODI score reduced to 6% since the first follow-up visit and remained stable up to the last follow-up at 15 months (Fig. 4). Along with a complete pain relief the patient experienced also a complete spasms relief at lower limbs, recovering from sensation of stiffness together with a significant functional improvement mostly related to walking ability, no longer needing assistance even for long-walking distances, therefore regaining confidence in walking. The level of muscle tone in each muscle group was assessed by Modified Ashworth Scale (MAS) scores in 3 joints of the patient’s lower and upper extremities with a 6-point (from 0 “No increase in muscle tone”, 1, 1+, 2, 3, to 4 “Affected parts rigid in flexion or extension”) scale. As shown in Fig. 5, the MAS scores of both legs gradually decreased, while no significant change was appreciated in the muscle tone of the upper extremities. Additionally, the change in painful symptoms compared with the baseline was assessed using the patient’s global impression of change (PGIC) Likert scale: relevant improvement of pain was achieved (“great and decisive improvement that makes the difference”) and improvement in the quality of sleep was reported. No perioperative complications or motor and sensory side effects during the follow up period were reported.
Fig. 3
Visual Analogue Scale (VAS) and Douleur Neuropathique en 4 Questionnaire (DN4) scores from baseline to 12-month follow-up
Fig. 4
Oswestry Disability Index (ODI) score from baseline to 12-month follow-up
Fig. 5
Modified Ashworth Scale (MAS) from baseline to 12-month follow-up
Indeed, all disabling and painful symptomatology in the upper limbs did not ameliorate and still represent a limitation.
留言 (0)