
記住我

Forty-nine subjects, 24 male and 25 female, were prospectively recruited to participate in this study. Inclusion criteria included age between 18- and 35-years. Exclusion criteria included back or hip pain, inability to stand upright or sit with hips flexed to 90°, a history of ankylosing spondylitis, femoroacetabular impingement, and prior hip or spine surgery. The present study was conducted as approved by the Institutional Review Board (IRB HS-22-00214).
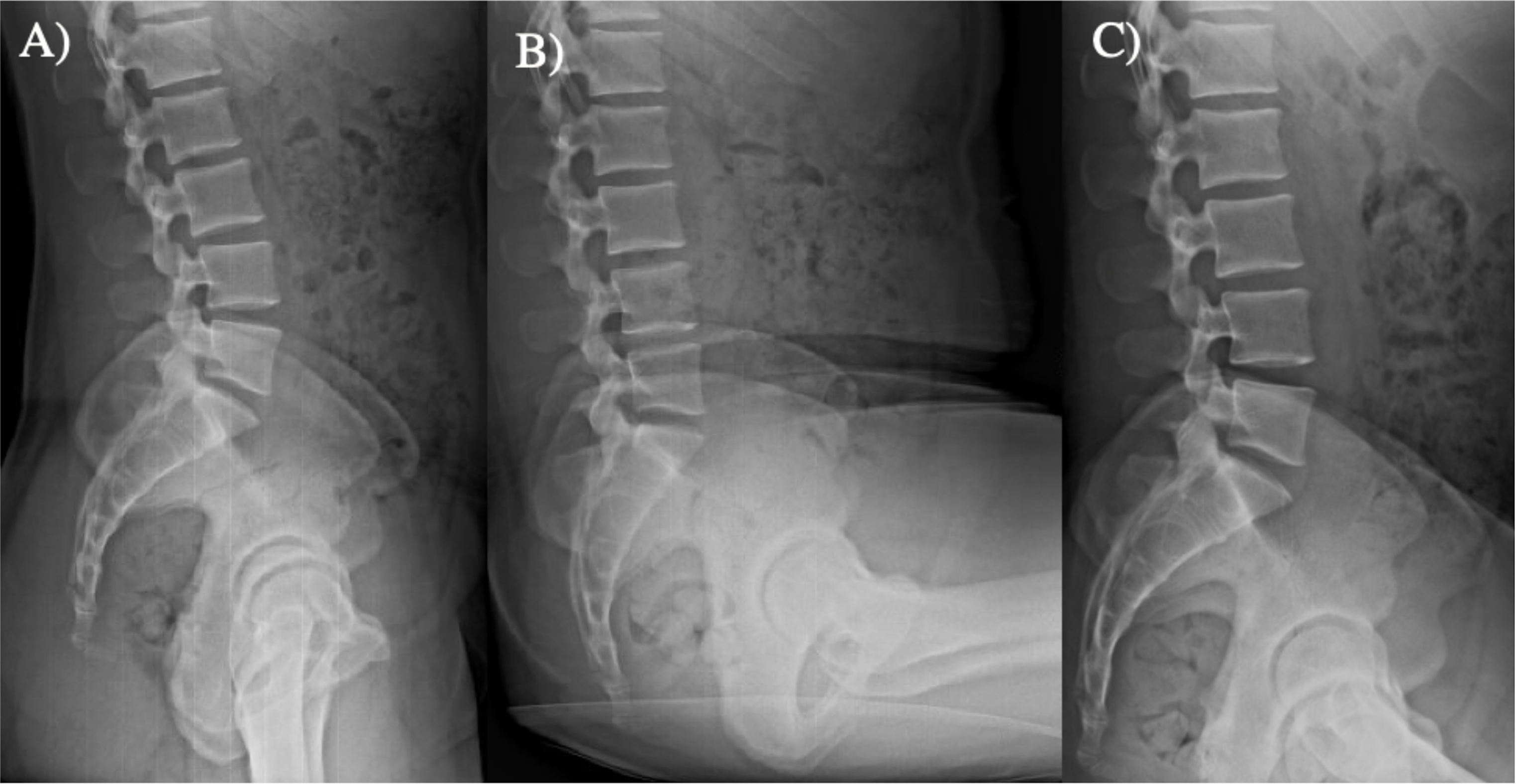
Three lateral radiographs were obtained for each subject: standing, relaxed-seated, and lateral decubitus. (Fig. 1) For the standing lateral radiograph, subjects were instructed to stand straight up and rested their arms on a bar in front of them with approximately 90° of shoulder flexion. For the relaxed-seated radiograph, subjects were instructed to sit down in a comfortable position with their hips and knees flexed to 90° with their hands resting on their knees. For the lateral decubitus radiograph, subjects were positioned in a lateral decubitus position on a table in the x-ray suite. To simulate intraoperative positioning, one pillow was placed under the head, two pillows were placed between the arms, and two pillows were placed between the legs. The arms and legs were positioned by a senior orthopaedic surgery resident (E.S.M.) and research staff to best approximate intraoperative positioning.
Fig. 1
(A) Standing (B) Seated and (C) Lateral Decubitus radiographs
Radiographic variables measured included LL, segmental lordosis at each lumbar level (L1-L2, L2-L3, L3-L4, L4-L5, L5-S1), pelvic incidence (PI), pelvic tilt (PT), and pelvic femoral angle (PFA) (Fig. 2) PFA is an established measure of hip flexion in the arthroplasty literature [17]. PI-LL mismatch was calculated as the difference between PI and LL. The lordosis change at each lumbar segment was calculated as the change in angle in the segment between a standing position and the lateral decubitus position. Each segment’s contribution to overall LL was calculated as the ratio of the individual segment divided by the overall LL.
Fig. 2
Radiographic measurements including (A) lumbar lordosis (angle between the superior endplate of L1 and then superior endplate of S1); (B) segmental lumbar lordosis (angle between inferior and superior endplate of each respective lumbar level); (C) pelvic incidence (the anterior-posterior dimension of the pelvis measured by the relationship between the femoral heads and the sacrum); (D) pelvic tilt (the difference between the pelvic incidence and the sacral slope); and (E) pelvic femoral angle (the angle of the femur relative to the sacrum)
Statistical analysisDescriptive statistics are reported as mean ± standard deviation. Pearson correlations were calculated to determine the correlation between various parameters. The correlations between standing LL and sitting LL compared to lateral LL were calculated. The correlations between standing PI, PT, PI-LL mismatch, SS, and LL and the change in LL when going from standing to lateral decubitus (ΔLL) were calculated to determine if there are any standing radiographic factors that correlated with an increased ΔLL. Finally, the correlation between PFA and LL in the lateral position was calculated. All statistics were completed using SPSS version 26 (IBM, Armonk, NY, USA). A p-value of < 0.05 was considered statistically significant.
留言 (0)