The use of a stent in hypospadias surgery aims to reduce both short and long-term post-operative complications; meatal stenosis, urethral fistula, and dehiscence being the principal issues that develop in 10% of distal and 33% of proximal primary repairs [4]. Various alternative methods of urine drainage after surgery have been described [1, 5, 6]. While some authors describe omission of this stent in hypospadias repair, the majority of surgeons opt to use various forms of drainage to bypass the urethroplasty.
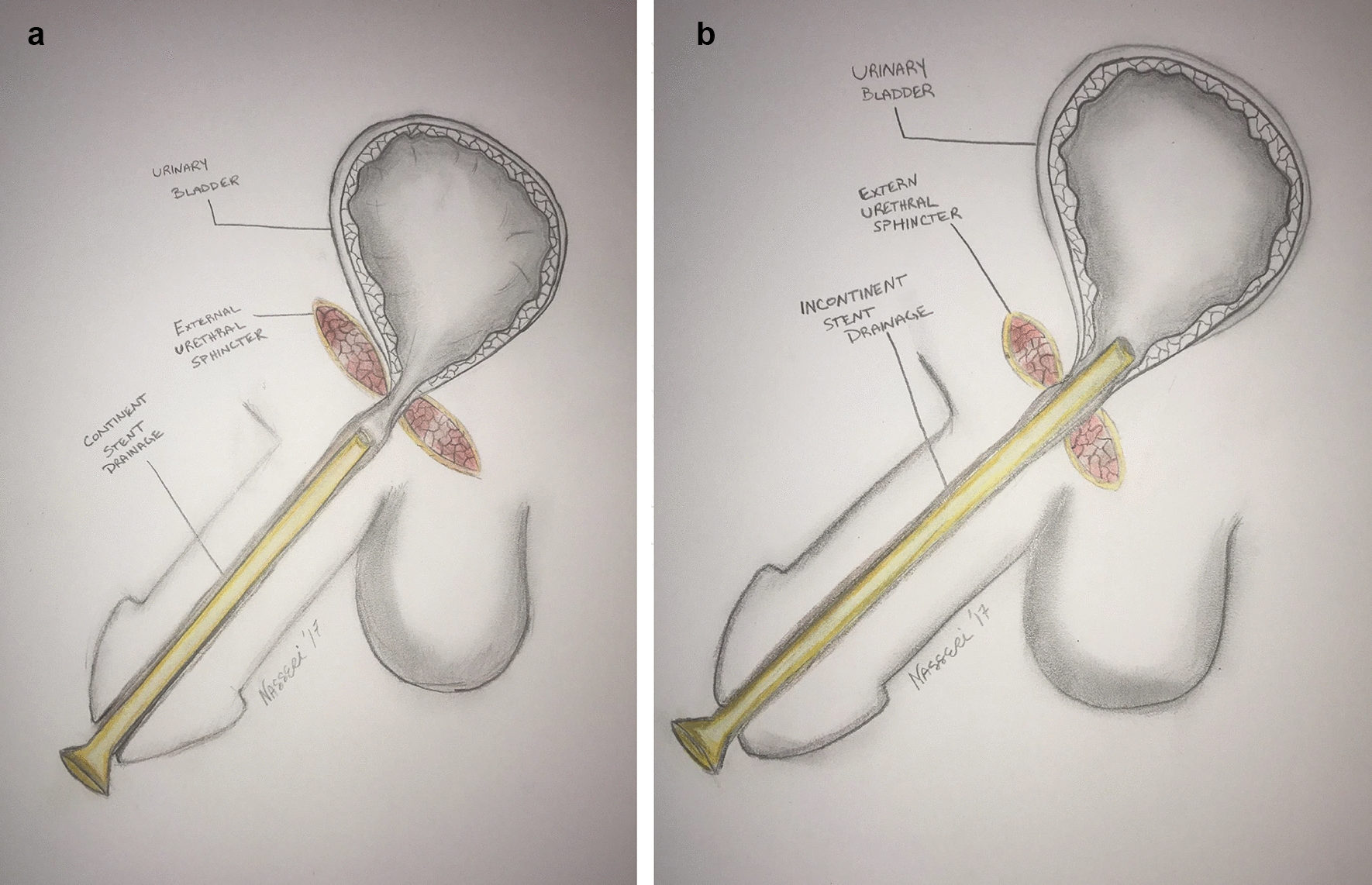
Buson et al. compared stented and non-stented patients undergoing meatal-based flap urethroplasty. A higher complication rate was observed in the non-stented group, with urinary retention developing in 19% of patients and urethrocutaneous fistula in 14% compared to 0–6%, respectively, in the stented group [7]. Another study stated that distal hypospadias patients could undergo surgery with no stent in toilet-trained children, but confirmed there were lower post-operative complications when a stent was used [8]. The use of a continent mid-urethral stent (MUS) was previously described. Mitchell et al. first reported the use of a urethral “splent” (silicone pleated stent) in 1986. None of the patients in this series required subsequent catheterization or hospitalization and urethral fistula developed in 4.5% of patients [9]. In our series urethral fistula developed in 13.5% in the “incontinent” group and only in 2.3% in the “continent” group.
Toilet-trained boys scheduled for hypospadias repair, both primary and secondary, represent a unique subgroup of hypospadias patients. Surgery alone has been proven a significant source of emotional trauma for the pediatric population [10]. While often only being for a limited period of time, the loss of continence experienced by children may be traumatic and may lead to discomfort in the post-operative period. Several studies have demonstrated the detrimental effects of long-standing incontinence with regard to quality of life and self-esteem. Children with nocturnal enuresis report lower self-esteem scores compared to continent children and show an improvement in self-esteem following treatment for this issue [11]. Gladh et al. observed that incontinent children 6–8 years of age suffer the greatest discrepancy in self-reported quality-of-life scores compared to continent children [12]. To the best of our knowledge, no existing literature has assessed the psychologic effects of temporary continence loss, especially due to iatrogenic causes, on quality of life.
An additional concern for the parents of boys with incontinent drainage following hypospadias surgery is the management of a catheter and leg bag or the subjecting their child to the discomfort of a diaper. Ambulation becomes cumbersome and the child’s active daily living can become restricted. Our method of continent drainage solves this issue. All patients in the “continent” drainage group were discharged on post-operative day 0 or 1 following repair, and 40/44 (91%) patients required no further management during their recovery period.
Although we did not report the rate of bladder spasms nor that of post-operative urinary tract infection in this study, it has been well-documented in other studies. Bladder spasm is commonly seen in toilet-trained boys following hypospadias repair. A meta-analysis performed by Mousavi et al. suggested that up to 30% of toilet-trained boys undergoing hypospadias repair complained of bladder spasm [13]. In a recent prospective, randomized trial, El-Karamany et al. reported a 47% rate of bladder spasms in toilet-trained boys who underwent hypospadias repair with a stent [14]. A continent MUS has potential to reduce symptoms aggravated by indwelling bladder drainage. We believe that further investigation is required to assess the efficacy of continent drainage in reducing bladder symptoms.
This cohort represents a relatively older group undergoing hypospadias repair. Furthermore, more than half (61%) of the patients in the “continent” stent group, and roughly half (52%) of patients overall were re-do cases of hypospadias repair. We believe that this may have resulted in a cohort at increased risk for complications in comparison to younger children undergoing primary repair. Kocherov et al. reported on their experience with 84 toilet-trained boys who underwent hypospadias repair with an overall complication rate of 27% [15]. Garnier et al. reported complications for patients undergoing primary hypospadias repair and noted that those over the age of two years at the time of surgery were at significantly higher risk of developing post-operative complications (OR 1.98, p = 0.002) [16]. Our study reported an overall complication rate of 25% and 17.7% requiring additional intervention. Regarding secondary repair and complication risk, Snodgrass et al. analyzed 1536 patients and reported that each prior attempted repair resulted in a 1.5-fold increase in complication risk (OR 1.51, CI 1.25–1.83) [4]. These studies describe findings which coincide with our own experience in a similar age group and reflect the complicated nature of hypospadias repair in older children.
At our institution, the use of MUS has become the standard of care for toilet-trained boys undergoing hypospadias repair. This modification holds potential advantages, not only for toilet-trained boys but also for non-toilet-trained boys undergoing the procedure. Furthermore, well designed studies focusing on younger non-continent boys are needed to explore the potential benefits of MUS in preventing bladder spasms and reducing post-operative complications such as urinary bladder infections. If proven beneficial, the widespread adoption of MUS in hypospadias repair could significantly improve outcomes for a majority of patients. However, the true benefit of this modification is yet to be studied and defined.
Our study is not without limitations. Data regarding pain, bladder spasms, and need for anticholinergic medication after surgery were not collected in this study. We did not address quality of life, ambulation limitations, or importantly, any regressive behavior that may have occurred after stent or catheter removal. These are significant questions to be answered and should be reported in future studies. We do believe, however, that in an appropriately selected patient, continent drainage offers advantages. For patients in whom there is little concern that bladder access may be lost, continent drainage may be utilized without additional risk of complications.


留言 (0)