
記住我





The present study was conducted between April 2014 and March 2016, involving a total of 264 cases from three different hospitals: Yueyang Hospital of Integrative Medicine affiliated with Shanghai University of Traditional Chinese Medicine (150 patients); Shanghai Hospital of Traditional Chinese Medicine (72 patients); and Shuguang Hospital affiliated to Shanghai University of Traditional Chinese Medicine (42 patients). These patients were suffering from rGERD. Patients from each of the three hospitals were randomly divided into treatment and control groups in a 1:1 ratio. Ultimately, the treatment group consisted of 132 patients, and the control group also included 132 patients. During the study period, a total of 22 patients were shed and the dislodgement rate was 8.33%, which included 11 lost to follow-up, 8 cases refused treatment, 2 patients left due to adverse events, and 1 case were pregnant (Tables 1and 2). There were no statistically significant differences in demographic characteristics (gender, age, BMI index), medical history data (type of PPI administration before enrollment, duration of PPI administration, concomitant medication for rGERD, allergic history, concomitant diseases, and treatment of concomitant diseases), as well as vital signs and physical examination results (Tables 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14).
Table 1 Distribution of case shedding and excluding in three centersTable 2 Case-specific causes of shedding and excludingTable 3 Comparison of gender composition between two groupsTable 4 Comparison of the age of patients in the two groupsTable 5 Comparison of obesity levels between the two groupsTable 6 Comparison of disease duration (months) between the two groupsTable 7 Comparison of the composition of the types of PPIs taken before enrollment between the two groupsTable 8 Comparison of the course of PPI administration before enrollmentTable 9 Comparison of comorbid medications prior to enrollmentTable 10 Comparison of allergy history between the two groupsTable 11 Comparison of concomitant diseases in the two groupsTable 12 Comparison of treatment of concomitant diseases in the two groupsTable 13 Comparison of vital signs between the two groups (FAS)Table 14 Comparison of the 7 major systems of physical examination between the two groups of patients (FAS)SHF combined with rabeprazole treatment improved clinical symptoms total efficacy of rGERD patientsAs the trends in the results of the FAS and PPS data analyses were essentially identical, the subsequent data analysis primarily relied on the FAS data analysis. WRS test showed that after 2 weeks of treatment, there was no significant difference in clinical efficacy between the treatment and control groups (Z = 0.248, P = 0.804). After 4 weeks, 6 weeks, and 8 weeks of treatment, there were statistically significant differences in clinical efficacy between the two groups (Z = 1.964, P = 0.050 at 4 weeks; Z = 2.054, P = 0.040 at 6 weeks; and Z = 9.422 at 8 weeks; P < 0.05; Table 15). Additionally, the results of the GEE analysis revealed a statistically significant difference between the treatment group and the control group (Wald χ2 = 25.657, P < 0.001). The clinical efficacy of the treatment group was significantly better than that of the control group. The repeated measurement ANOVA (rmANOVA) also revealed significant differences in clinical efficacy between the two groups at various time points, including 2 weeks, 4 weeks, 6 weeks, 8 weeks treatments (Wald χ2 = 272.697, P < 0.001). Notably, the clinical efficacy became increasingly pronounced as the treatment duration extended in two groups (Table 16).
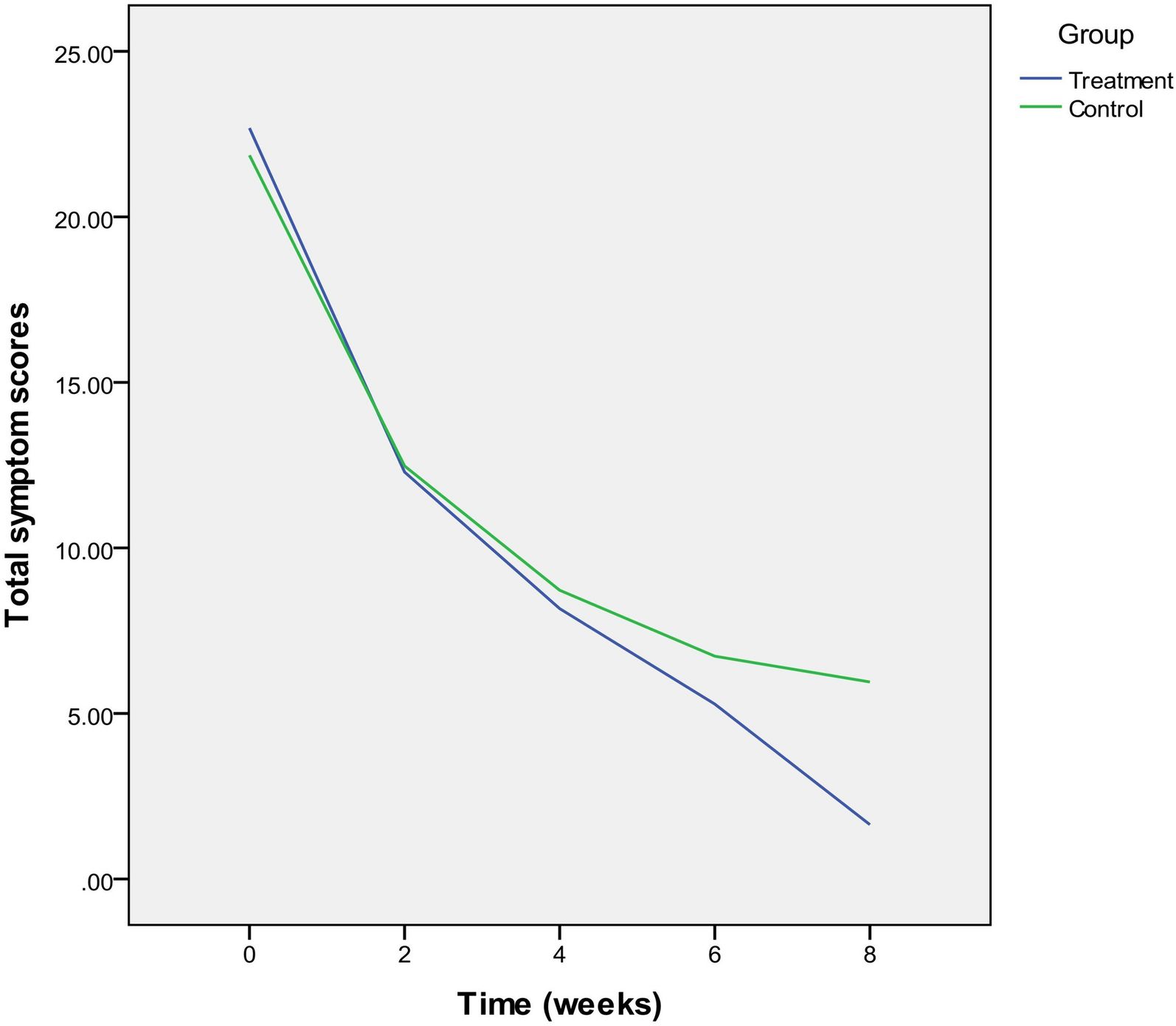
Table 15 Comparison of efficacy between the two groups at different times (FAS)Table 16 Generalized estimating equation to estimate the total efficacy of clinical symptoms (FAS)SHF combined with rabeprazole treatment reduced total symptom scoresThere were no differences in total symptom scores between the treatment and control groups before interventions (F = 0.549, P = 0.459), suggesting the same baseline between the two groups. WRS test showed that there was a statistically significant difference between pre-treatment and 8 weeks of treatment in both the treatment group (F = 435.172, P < 0.001) and the control group (F = 322.442, P < 0.001). At 6 weeks of treatment (F = 5.579, P = 0.019) and 8 weeks of treatment (F = 74.490, P < 0.001), a statistically significant difference emerged between the two groups, with the treatment group demonstrating superiority over the control group (Table 17). Results from the rmANOVA analysis indicated a statistically significant divergence between the total clinical symptom scores of all patients before and after treatment (F = 752.547, P < 0.001). Furthermore, there was an interaction between time and group (F = 13.565, P < 0.001; Table 18). Based on the graph, both the treatment group and the control group showed a similar decreasing trend in total clinical symptom scores before, after 2 weeks, and after 4 weeks treatment. However, the treatment group exhibited a faster reduction in total clinical symptom scores at 6 weeks and 8 weeks of treatment (Fig. 1).
Table 17 Comparison of total symptom scores between the two groups at different treatment times (FAS)Table 18 Repeated measures ANOVA results of total clinical symptom scores in the two groups (FAS)Fig. 1
Trends in total clinical scores at different times in two groups (FAS)
SHF combined with rabeprazole treatment reduced major symptom scoresSubsequently, we investigated the impact of SHF on primary symptoms of rGERD, which encompassed heartburn, retrosternal pain, regurgitation and belching, and acid regurgitation. Before the interventions, there were no differences in these main symptoms between the treatment and control groups (P > 0.05), which indicated that baseline was same for both groups. WRS test showed that after 2 weeks, 4 weeks, and after 6 weeks of treatment, there was no statistically significant difference in these main symptoms between the two groups (P > 0.05). After 8 weeks of treatment, a statistically significant difference was observed in these main symptoms between the two groups of patients (P < 0.05). Based on the mean rank, it could be concluded that the treatment group exhibited superior efficacy in managing these main symptoms compared to the control group. The results of the GEE analysis showed that there was no statistically significant difference between the treatment and control groups in the main symptom scores of heartburn, retrosternal pain, regurgitation and belching, and acid regurgitation after 8 weeks of treatment (P > 0.05). Furthermore, compared with pre-treatment, the results of the rmANOVA revealed statistically significant differences in these symptom scores both in the two groups after 2 weeks, 4 weeks, 6 weeks, and 8 weeks of treatment (P < 0.05). Moreover, as the treatment duration increased, both groups showed improved treatment effects (Tables 19, 20, 21, 22, 23, 24, 25and26).
Table 19 Comparison of the degree of heartburn in the two groups at different times (FAS)Table 20 Generalized estimating equations results of heartburn score (FAS)Table 21 Comparison of the degree of retrosternal pain in the two groups at different times (FAS)Table 22 Results of generalized estimation equation for estimating retrosternal pain (FAS)Table 23 Comparison of the degree of regurgitation and belching between two groups of patients at different times (FAS)Table 24 Results of generalized estimation equation for estimating regurgitation and belching (FAS)Table 25 Comparison of the degree of acid regurgitation in the two groups at different times (FAS)Table 26 Results of generalized estimation equation for estimating acid regurgitation (FAS)SHF combined with rabeprazole treatment improved reflux esophagitisWRS test showed that there were no differences in the incidence of reflux esophagitis between the treatment and control groups prior to the interventions (F = 0.129, P = 0.897), indicating that all groups had the same baseline. After 8 weeks treatment, there was no statistically significant difference in the severity of reflux esophagitis between the two groups (F = 1.410, P = 0.159; Table 27). After 8 weeks of treatment, compared with pre-treatment, there was a statistically significant difference in the both the treatment (Z = 8.169, P < 0.001) and control groups (Z = 9.800, P < 0.001; Table 28). Analysis based on the FAS indicated that in the treatment group, patients with esophagitis grade A decreased from 40.34% to 17.23%, and those with grade B decreased from 11.76% to 3.78%. In the control group, patients with esophagitis grade A decreased from 40.25% to 15.35%, and those with grade B decreased from 11.20 to 2.49% (Fig. 2). This suggested that both groups exhibited similar efficacy in improving the degree of esophageal inflammation.
Table 27 Comparison of severity of reflux esophagitis between the two groups at different timesTable 28 Comparison of reflux esophagitis in the treatment and control groups before treatment and at 8 weeks of treatmentFig. 2
Distribution of esophagitis types (FAS) before and after treatment in both groups
SF-36 scale reliability analysisSF-36 was used to assess quality of life for patients with rGERD. The assessment of the SF-36 scale's reliability revealed that the Cronbach's α for the pre-treatment scale exceeded 0.8, indicating a high level of reliability in the researcher's evaluation of the patients' health status. In the case of the post-treatment scale, Cronbach's α exceeded 0.8 across all groups, with the exceptions of 0.796 in the control group at the Shanghai Hospital of Traditional Chinese Medicine and 0.761 in the treatment group at Shuguang Hospital. This suggested that the researcher's second assessment of the patients' health status following treatment remained highly reliable. The combined Cronbach's α for the pre-treatment assessments was 0.900, while for the post-treatment assessments, it was 0.877 (Table 29).
Table 29 Reliability analysis of the SF-36 scale for patients (FAS)SHF combined with rabeprazole treatment improved the quality of life of patients with rGERDBefore interventions, there were no differences in the scores of each indicator between the treatment group and the control group (P > 0.05). In terms of all eight evaluation dimensions, both groups exhibited a significant improvement in patients' quality of life after 8 weeks of treatment compared to before treatment (P < 0.05; Table 30). Furthermore, rmANOVA showed that after 8 weeks of treatment, the treatment group demonstrated a significantly greater improvement in quality of life compared to the control group (P < 0.05). Additionally, there was a significant interaction between time and group for PF, RP, VT, BP, and RE (P < 0.05), suggesting that the scores in these five dimensions increased more rapidly with prolonged treatment. Statistically, the treatment group outperformed the control group in terms of RP, VT, and GH (P < 0.05; Table 31), indicating that scores in the treatment group improved more significantly over time compared to the control group.
Table 30 Comparison of the dimensions of the SF-36 scale between the two groups (FAS)Table 31 Results of repeated measurement ANOVA for SF-36 dimension (FAS)SHF combined with rabeprazole treatment increased total somato-physical health and psychiatric mental health scoresWRS test showed that there was no statistical difference between the two groups at the pre-treatment in terms of total scores for somatic-physical health (F = 0.954, P = 0.330) and psychiatric mental health (F = 0.817, P = 0.367), allowing for follow-up comparisons. Both groups significantly improved their scores on somato-physical health and psychiatric mental health scores after 8 weeks of treatment compared to pre-treatment (P < 0.05; Figs. 3and4). Additionally, following 8 weeks of treatment, there were also statistically significant differences in scores between the two groups (P < 0.05). Based on the mean values, the treatment group was superior to the control group. The rmANOVA showed that all patients had significantly higher somato-physical health and psychiatric mental health scores after 8 weeks of treatment compared to pre-treatment (P < 0.05). There was an interaction between time and group (F = 17.909, P < 0.001), suggesting that the total somato-physical health and psychiatric mental health scores gradually increased with the prolongation of treatment. After 8 weeks of treatment, the treatment group was significantly faster than the control group in rising scores (Tables 32, 33, 34and35).
Fig. 3
Time and group interaction plot for somato-physical health scores (FAS)
Fig. 4
Time and group interaction plot for psychiatric mental health scores (FAS)
Table 32 Comparison of total somato-physical health scoresTable 33 Repeated measurement ANOVA of somato-physical health scoresTable 34 Comparison of total psychiatric mental health scoresTable 35 Repeated measurement ANOVA of psychiatric mental health scoresCharacteristics of the first symptoms of rGERD in Chinese medicineTwo hundred and sixty-four patients diagnosed with rGERD based on Chinese medicine evidence were subjected to systematic cluster analysis using Ward's method and Euclidean distance. The analysis revealed five distinct categories based on the degree of symptom similarity (Fig. 5). Further analysis by gender yielded consistent results, suggesting that patients with rGERD could be classified into five categories (Fig. 6).
Fig. 5
Cluster diagram of Ward method sample system for all rGERD patients
Fig. 6
Cluster diagram of Ward method sample system for rGERD patients of different genders
Cluster analysis of indicator systemUsing systematic cluster analysis with Ward's method and Euclidean distance, we categorized the primary and secondary symptoms of 264 patients with rGERD based on their initial visit to a Chinese medicine doctor. The analysis identified two categories of symptoms. The first category included symptoms such as heartburn (SX), acid reflux (FS), retrosternal pain (XGHTT), regurgitation belching (FWAQ), dry mouth and bitter mouth (KGKK), and the sensation of pharyngeal obstruction (YBGZG). The second category comprised symptoms like dysphagia (TYKN), dyspareunia (NC), constipation (BM), loose bowel movements (BT), fatigue (SPFL), coldness and limb discomfort (WHZL), cough (KS), dry and sore throat (YGYT), epigastric pain (SFT), abdominal distension (FZ), and heartburn-induced insomnia (XFSM; Fig. 7).
Fig. 7
Systematic clustering of Ward's method indicators for all rGERD patients
Gender-based cluster analysis revealed distinct patterns in symptom grouping. Among male patients, symptoms such as heartburn (SX), acid reflux (FS), retrosternal pain (XGHTT), regurgitation, belching (FWAQ), pharyngeal obstruction sensation (YBGZG), and abdominal distension (FZ) were clustered together. In contrast, female patients exhibited a different pattern, with heartburn (SX), pantothenic acid (FS), pharyngeal obstruction sensation (YBGZG), dry pharynx, sore throat (YGYT), fatigue (SPFL), and distraction-induced insomnia (XFSM) forming a distinct symptom cluster. These findings indicated some variation in symptom grouping between the two genders (Fig. 8).
Fig. 8
Clustering diagram of the Ward method indicator system for patients of different genders
The grading of symptom severity during the patient's initial visitThe primary symptoms observed during the initial visit of patients with rGERD, ranked in descending order based on the severity composition ratio (Table 36), were as follows: regurgitation and belching (25.4%), retrosternal pain (20.8%), acid reflux (14.4%), and heartburn (13.6%). When considering the composition ratio of moderate and severe cases, the order of prevalence was as follows: regurgitation and belching (59.9%), acid reflux (46.2%), heartburn (44.3%), and retrosternal pain (40.5%).
Table 36 Grading of the severity of Chinese medicine symptoms in the first consultation of patients in the three centersAmong the other symptoms in patients with rGERD, the top five in terms of severity included dry mouth and bitterness (26.9%), pharyngeal obstruction (25.0%), insomnia and heartburn (16.7%), abdominal distension (15.9%), and fatigue (14.4%). When considering the component ratios of moderate and severe cases, the top five included dry mouth (53.0%), pharyngeal obstruction (48.9%), bloating (41.7%), insomnia (38.7%), and fatigue (35.5%).
Safety assessmentResearch has demonstrated that certain Chinese herbal medicines may have adverse effects on liver and kidney function. In this study, we assessed the incidence of abnormalities in ALT, AST, BUN, Cr, WBC, urinalysis, fecal routine, electrocardiogram in both groups. The results indicated that there was no statistically significant difference in the incidence of abnormalities in these parameters before treatment and after 8 weeks of treatment within each group (P > 0.05). Furthermore, when comparing the treatment group to the control group, there was no statistically significant difference in the incidence of abnormalities before treatment and after 8 weeks of treatment (P > 0.05).
Adverse eventsAmong the 264 subjects, adverse events were reported in 9 cases at Yueyang Hospital, with 3 cases in the treatment group and 5 cases in the control group. At Shuguang Hospital, there was 1 case in the treatment group. Out of these 9 patients, 1 patient was removed from the clinical trial due to a suspected drug-related adverse reaction, while the other 2 were removed from the trial due to other medical conditions necessitating treatment.
留言 (0)