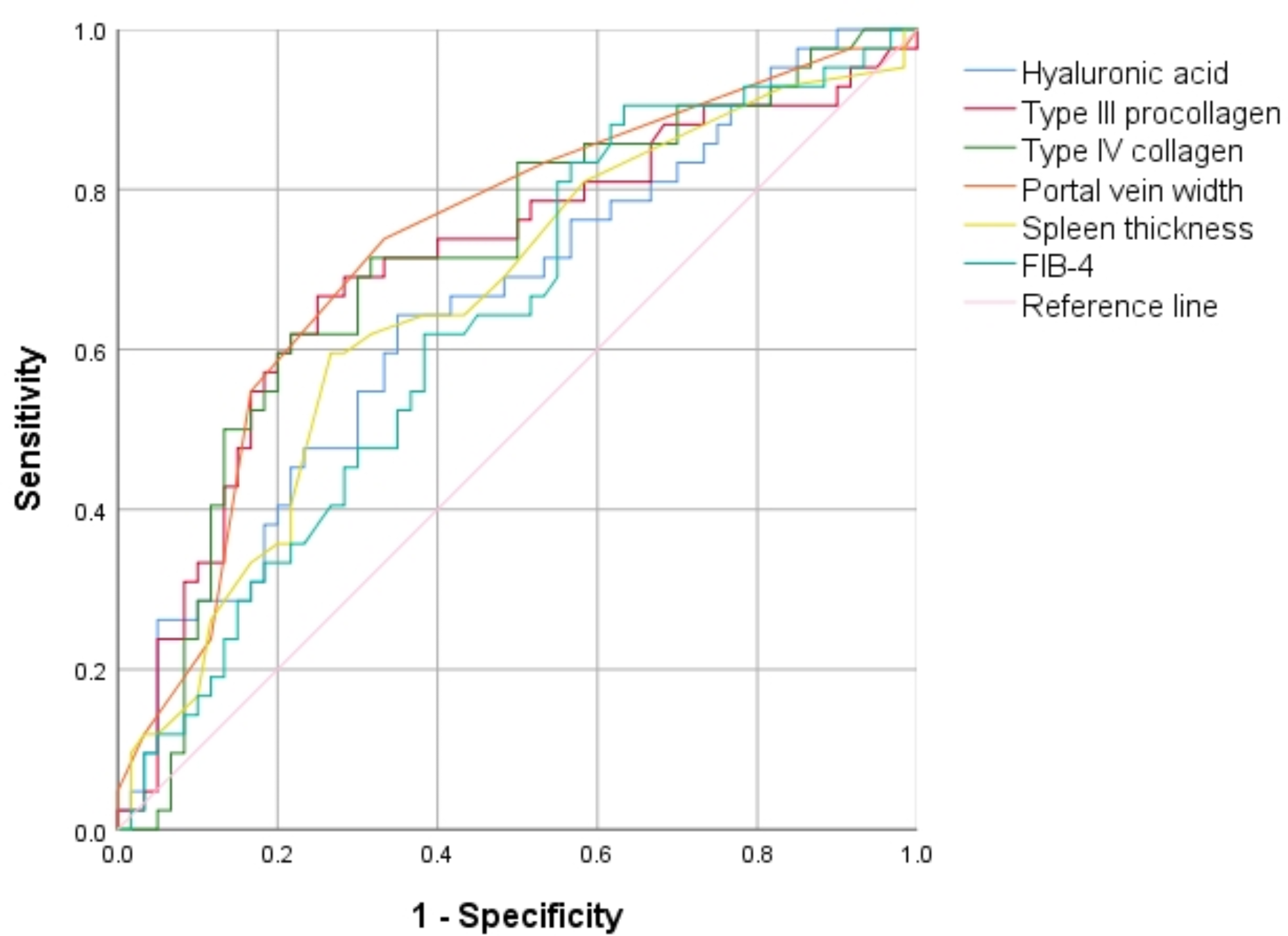
EVB constitutes a common and severe complication often encountered in patients with liver cirrhosis. EVB manifests with sudden onset, rapid deterioration, and a significantly heightened fatality rate. Despite its gravity, there exists a conspicuous absence of effective predictive models or systems for assessing EVB risk in clinical settings. In recent years, there has been a surge of interest in noninvasive index prediction of EVB within academic circles [10]. In this study, we conducted a comparison among various noninvasive serum liver fibrosis indicators, including but not limited to HA, PC-III, IV-C, Child-Pugh stage, AAR, APRI, FIB-4, PVD, and SPT.
Patients diagnosed with cirrhosis were categorized into two groups, namely the P group (without EVB) and the PE group (with EVB). Presently, a variety of methods are employed to assess the risk and prognosis of EVB, with noninvasive markers being particularly emphasized [11, 12]. In this study, a univariate analysis was undertaken, revealing notable differences in HA, PC-III, IV-C, PVD, SPT, and FIB-4 between the aforementioned groups. Recent studies have demonstrated that the stage of liver cirrhosis, when combined with hepatic venous pressure gradient, may predict the likelihood of EVB [13]. Nonetheless, invasive procedures are often poorly tolerated by patients and are not universally applicable. Employing binary logistic regression, we integrated these variables, constructed the ROC curves, and computed the AUROC. Our findings indicate that a composite of liver fibrosis indicators, comprising HA, PC-III, IV-C, and PVD, exhibits the highest diagnostic efficacy for EVB.
Liver fibrosis, a pathological state, manifests through an abnormal accumulation of extracellular matrix elements within the liver, potentially progressing into decompensated cirrhosis if left unaddressed, leading to severe health ramifications. In contemporary medical practice, indicators like HA, PC-III, and IV-C are routinely utilized to gauge cirrhosis severity.
Extensive research highlights the exceptional effectiveness of HA in precisely determining the extent of liver cirrhosis [14, 15]. Elevated concentrations of HA are consistently observed during both the active and advanced stages of liver disease, highlighting its potential close association with the progression of liver fibrosis. This is evidenced by the positive correlation between HA levels and the severity of fibrosis [16].
PC-III, derived from both hepatocytes and interstitial cells, is present in the bloodstream. Evaluating serum PC-III levels provides insight on the synthesis of collagen by hepatocytes. As an amino-terminal polypeptide, PC-III acts as a precursor to type III collagen, which is prevalent in the early phases of liver fibrosis. Thus, monitoring PC-III provides critical insights into the metabolism of type III collagen during these early fibrotic processes. Research findings indicate that PC-III is a promising metric for the assessment of liver fibrosis [17, 18].
IV-C, a key component of the hepatic basement membrane, exhibits escalated synthesis subsequent to liver injury, potentially functioning as a marker for the severity of liver fibrosis. Previous studies have revealed a significant positive correlation between serum levels of HA and IV-C among patients, along with the extent of esophageal varices [19]. Prior investigations have demonstrated a direct correlation between HA levels and the severity of esophageal varices [20, 21].
Hence, the elevation in serum levels of these markers likely mirrors the advancement of liver cirrhosis and the extent of esophageal varices, indicative of a heightened risk of bleeding commensurate with the severity of the varices. Moreover, in this study, no significant variances in age or Child-Pugh classification were discerned between the two groups.
Prior studies have scrutinized the risk factors for EVB in cirrhotic patients. Findings suggest that factors such as gender and age exhibit minimal correlation with EVB, while a higher Child-Pugh score demonstrates a notable association with its incidence. However, it is important to note that, despite its correlation with the incidence of EVB in cirrhosis, the Child-Pugh classification does not constitute an independent risk factor and possesses limited clinical significance in the prognostic assessment of EVB [22].
PH is a prominent clinical manifestation of liver cirrhosis, significantly impacting mortality rates among afflicted individuals [23]. PVD acts as an indirect gauge of PH severity, with higher PVD levels correlating with more pronounced EV and heightened susceptibility to EVB. Measurements obtained through real-time shear wave elastography in patients with cirrhosis have shown a direct relationship between PVD and the severity of EV, indicating that an increase in PVD is associated with more severe cases of EV. Enhanced MRI has demonstrated potential in predicting PH and identifying high-risk EV in patients with cirrhosis due to hepatitis B, highlighting the association between PV characteristics and EVB risk. Integrating MRI with PVD measurement, as evidenced in studies conducted in China, offers a comprehensive approach for assessing severe EV, demonstrating high diagnostic efficacy. Numerous studies have independently verified PVD as a significant risk factor for EVB and subsequent rebleeding events.








留言 (0)