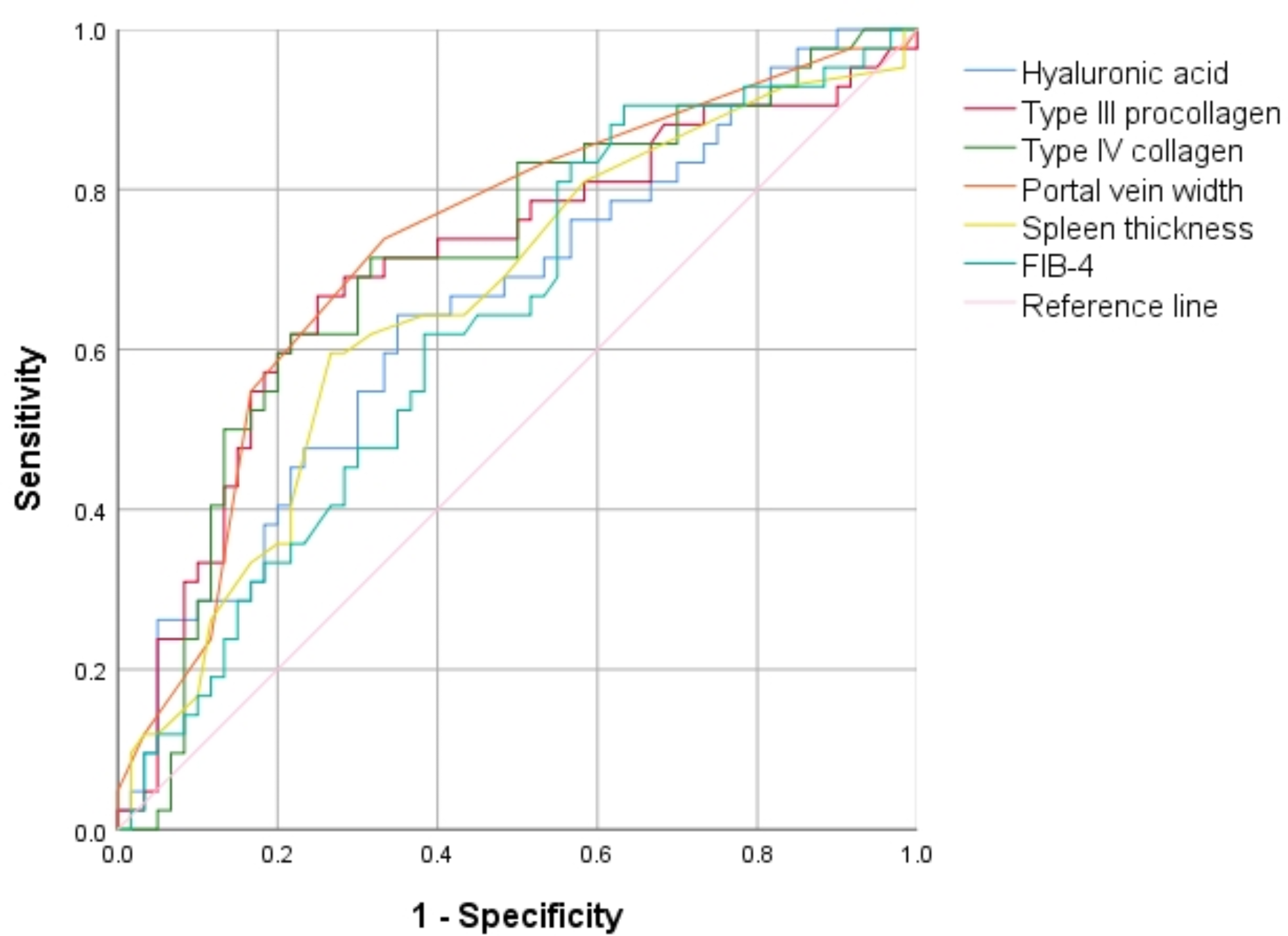
In this prospective study we reported the comprehensive analysis of iron metabolism indexes after cardiac surgery. We found that levels of S-Fe, unlike other iron related metabolism indicators, rose in AKI group. we also examined the ability of S-Fe to predict postoperative AKI by ROC curve. Furthermore, we combined S-Fe and APACHE II score to plot ROC curve to predict CSA-AKI. These findings support the notion that S-Fe levels may be an indicator of poor outcomes after cardiac surgery.
Iron is an essential microelement for the human body, which plays an active role in maintaining physiological functions. During CPB, red blood cells are exposed to nonphysiologic surfaces, shear forces may injure red blood cells, leading to the release of free hemoglobin and catalytic iron [9]. During aortic cross-clamp and reperfusion period, the levels of catalytic iron increase, which could contribute to oxidative stress and cellular damage, resulting in tubular necrosis [10]. After cardiac surgery, a large amount of catalytic iron is released, which may trigger AKI and mediate death [8]. Some studies found that elevated plasma catalytic iron levels are independently associated with increased prevalence of AKI after cardiac surgery [9, 17]. We found that patients who developed CSA-AKI had longer CPB time, longer aortic cross-clamp time. Adding to these findings, in this study we reported that patients who developed AKI had elevated serum catalytic iron levels upon admission to the ICU.
Ferritin is the primary tissue iron-storage protein, and may release iron in the presence of superoxide produced under conditions of inflammation [18]. Ferritin consists of 24 subunits of heavy (FtH) and light (FtL) chains. FtH can convert ferrous iron into ferric iron, which is stored within the ferritin shell subsequently [19]. The level of serum ferritin can indirectly reflect the level of FtH in the body. Nora Choi et al. found that patients with higher baseline serum ferritin levels have a low probability of developing CSA-AKI [12]. It is further suggested that high serum ferritin levels can reflect the body’s immunoregulatory capacity and ability to process catalytic iron release during CPB. We found no significant difference in the serum ferritin levels between the AKI group and non-AKI group. Because we only included data at the time of ICU admission, we did not collect the data of preoperative serum ferritin levels.
TRF is produced in the liver and binds one or two Fe3+ atoms in the circulation, and therefrom endocytosed by a variety of cells through specific plasma membrane receptors (TfR1 and TfR2). TRF is known to be filtered through the glomerular filtration barrier, and reabsorbed in the proximal tubule [20]. Increased urinary excretion of TRF results from decreased tubular uptake. Some studies show that urinary TRF can be further explored as a wider biomarker of renal damage induced by insults causing subclinical tubular alterations, which means that high levels of TRF may predict a higher incidence of AKI [20]. Iron binding capacity is the capacity of TRF to bind with iron. There are two types of iron binding capacity, TIBC and UIBC. As only one-third of TRF is saturated with iron, so the TRF present in serum has an extra binding capacity (67%), which is called UIBC. TIBC was calculated as the sum of the serum iron plus the UIBC [21]. TS was calculated as the percentage of iron to total iron binding capacity. Choi N et al. found that TS elevated at 1 h after CPB, which can be used as an independent predictor of the incidence of AKI after cardiac surgery [12]. sTfR is derived from proteolysis of the membrane transferrin receptor, it can be used to assess iron status. sTfR has been widely used in cardiopulmonary disease research [22]. Frise et al. found that when defined using sTfR rather than ferritin, non-anemic iron deficiency predicts prolonged hospitalisation following surgical aortic valve replacement [23]. Choi N et al. found that lower serum ferritin and higher transferrin saturation at 1 h CPB were independent predictors of acute kidney injury [12]. Lower intraoperative iron-binding proteins are inversely associated with postoperative AKI development, suggesting an impaired capacity to rapidly handle free iron release during CPB leading to AKI. However, we found no statistically significant difference in TRF, UIBC, TIBC, TS and sTfR between the two groups.
There are several limitations in our study. First, the sample size of our study is relatively small, so the level of evidence provided by our study is not high enough. However, Nora Choi, et al. conducted a study, the base clinical prediction model (Thakar score) demonstrated good discrimination for CSA-AKI (AUC, 0.72; 95% CI, 0.62–0.81), the intraoperative model (Thakar score, serum ferritin, and TS) is better clinical prediction alone (AUC, 0.76; 95% CI, 0.67–0.85) [12]. Second, we did not take urine volume into consideration as done in the previous study, because some patients were treated with diuretics and the urine volume is inaccurate, which may result in bias. Third, we did not study the relationship between the patient's preoperative iron metabolism indexes and CSA-AKI. However, we found no difference in preoperative haemoglobin between the two groups. We plan to study the role of preoperative and postoperative iron metabolism indexes in the more crowds and explore the mechanism between ferroptosis and CSA-AKI in the future.
The results of our study and other researches highlight the importance of iron homeostasis in human ischemia–reperfusion injury and suggest it is a potentially modifiable risk during cardiac surgery [12]. Given that ferroptosis is extensively involved in the occurrence and development mechanisms of CSA-AKI, targeting the ferroptosis pathway may be a novel strategy for preventing and treating AKI. This strategy mainly includes iron chelation therapy, targeting iron metabolism-related proteins, lipophilic antioxidants, and direct inhibitors of ferroptosis [24]. What is more, further researches are required to verify these results.








留言 (0)