
記住我






At the time of analysis, data from 912 patients were included in the study. Table 1 provides a summary of the characteristics of these patients.
Table 1 General characteristics of the ASRI cohortWithin the ASRI cohort, 685 patients (75.1%) were male. The median age of the participants was 44 years, and the median age at the onset of the first Axial Spondylarthritis (AxSpA) symptom was 25 years. The average disease duration among the participants was 16 years.
A majority of the patients, 694 (76.1%), met the modified New York (mNY) criteria for radiographic AxSpA (rAxSpA), while 733 patients (84.9%) were found to be HLA-B27 positive. Frequently reported EMMs included uveitis (34.4%), psoriasis (16.8%), inflammatory bowel disease (10.7%), and depression (10.4%).
In terms of treatment, the most frequently administered therapies were tumor necrosis factor (TNF) inhibitors (58.2%) and non-steroidal anti-inflammatory drugs (NSAIDs), which were used by 51.1% of participants. 30.2% of participants were receiving multiple treatment options, while 13.9% were not receiving any treatment.
Features associated with PA and dactylitisOut of the 912 patients, 276 participants (30.9%) reported peripheral arthritis (PA), while 60 patients (6.6%) had dactylitis. Table 2 provides a summary of the characteristics associated with these peripheral manifestations.
Table 2 Characteristics of AxSpA patients with peripheral arthritis and/or dactylitisThere was a strong association between peripheral arthritis and dactylitis within the cohort. Among the 60 patients with dactylitis, 42 (70%) also presented with peripheral arthritis, indicating a significant overlap between the two conditions (OR 6.31).
In univariate analysis, both peripheral arthritis (OR 0.68, P = 0.019) and dactylitis (OR 0.38, P = 0.003) were inversely associated with male sex. Peripheral arthritis was associated with older patient age (48 vs. 44 years, P < 0.001) and longer AxSpA duration (19 vs. 15 years, P < 0.001). However, no relationship was observed between dactylitis and either age or AxSpA disease duration.
Patients with PA or dactylitis had worse BASDAI scores compared to those without these peripheral features (PA: 4.4 vs. 3.6, P < 0.001; dactylitis: 5.6 vs. 3.5, P < 0.001). These associations remained robust in multivariate regression analysis. Peripheral arthritis, but not dactylitis, showed residual association with worse scores in BASFI (3.7 vs. 2.9, P = 0.005), AsQoL (7 vs. 4, P = 0.002), and HAQ-s (0.5 vs. 0.4, P < 0.001), after accounting for covariates in multivariate analysis.
Among the EMMs, psoriasis was more frequent in patients with both PA (OR 2.2, P < 0.001) and dactylitis (OR 3.38, P < 0.001). However, while dactylitis showed a strong association with uveitis (OR 2.91, P < 0.001) and inflammatory bowel disease (IBD) (OR 3.15, P < 0.001), PA did not show a significant association with either of these manifestations after accounting for covariates. PA was associated with accompanying depression (OR 1.79, P = 0.012), which remained significant after accounting for covariates.
Therapeutic options chosen by clinicians differed based on the presence of PA and dactylitis in patients. Methotrexate was more commonly administered to patients with PA (OR 4.93, P < 0.001) and/or dactylitis (OR 4.32, P = 0.001). Peripheral arthritis was also associated with the administration of sulfasalazine (OR 2.31, P = 0.03) and multiple drug treatments (OR 1.95, P < 0.001). While sulfasalazine and multiple therapies were also, to a lesser degree, more commonly administered to patients with dactylitis (OR 1.47 and 1.29, respectively), these findings were not statistically significant.
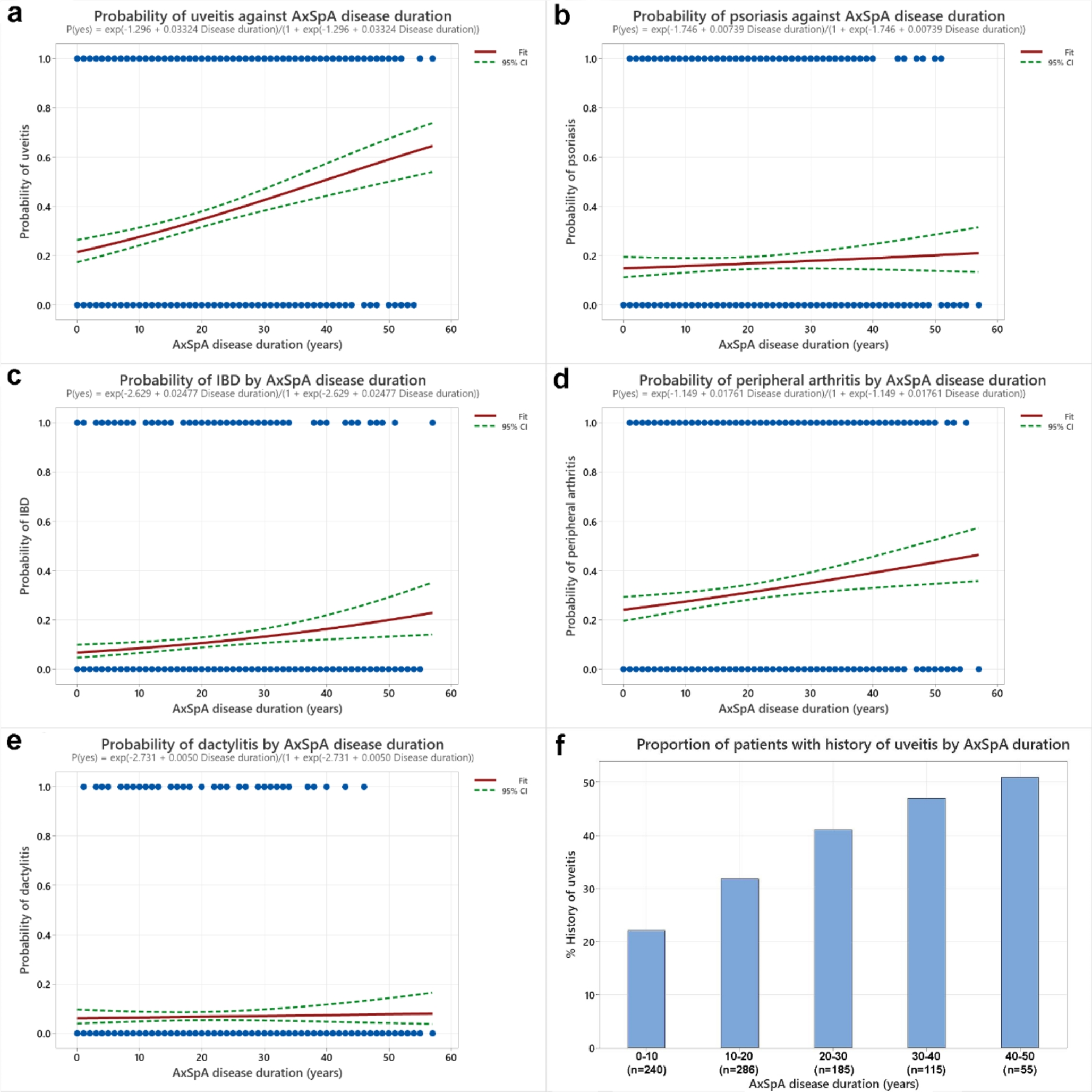
Peripheral arthritis but not dactylitis is associated with AxSpA disease durationDue to the lack of specific dates when peripheral manifestations developed in patients, we employed logistic regression to model the presence or absence of these manifestations against AxSpA disease duration. The results of this analysis are presented in Fig. 1 (a-e).
All of uveitis, peripheral arthritis, and inflammatory bowel disease (IBD) showed a positive association with AxSpA disease duration. Particularly, uveitis exhibited a notable trend, with its prevalence reaching 50% after 40–50 years post-AxSpA onset (Fig. 1f). In contrast, both psoriasis and dactylitis demonstrated no significant association with AxSpA disease duration, suggesting that these features tend to either precede or develop shortly after AxSpA onset.
Fig. 1
(a-e) Binary logistic regression of peripheral features against AxSpA disease duration. Trend indicated in red; dashed lines represent 95% confidence interval. (f) Bar chart representation of the proportion of patients with a history of uveitis against AxSpA disease duration
留言 (0)