In this study, we compared PA measurements in patients with HFrEF with those of age- and sex-matched healthy controls. Additionally, in patients with HF, we investigated the relationships between PA measurements and established markers of physical capacity and prognosis. This study produced several main findings: first, the repeatability of PA measurements was high. Second, the daily PA in patients with HFrEF was severely reduced compared with that of healthy controls, and the time spent in MVPA represented a key difference between the PA of patients with HF and that of healthy controls. Third, in patients with HF, we found only moderate correlations between accelerometer measurements, peak VO2, and 6MWD; and no significant correlations with other traditional HF prognostic markers, such as LVEF and NT-ProBNP. Finally, a low PA phenotype among patients with HF was characterised by poor physical capacity.
Physical activity measurements in patients with heart failure and healthy controls
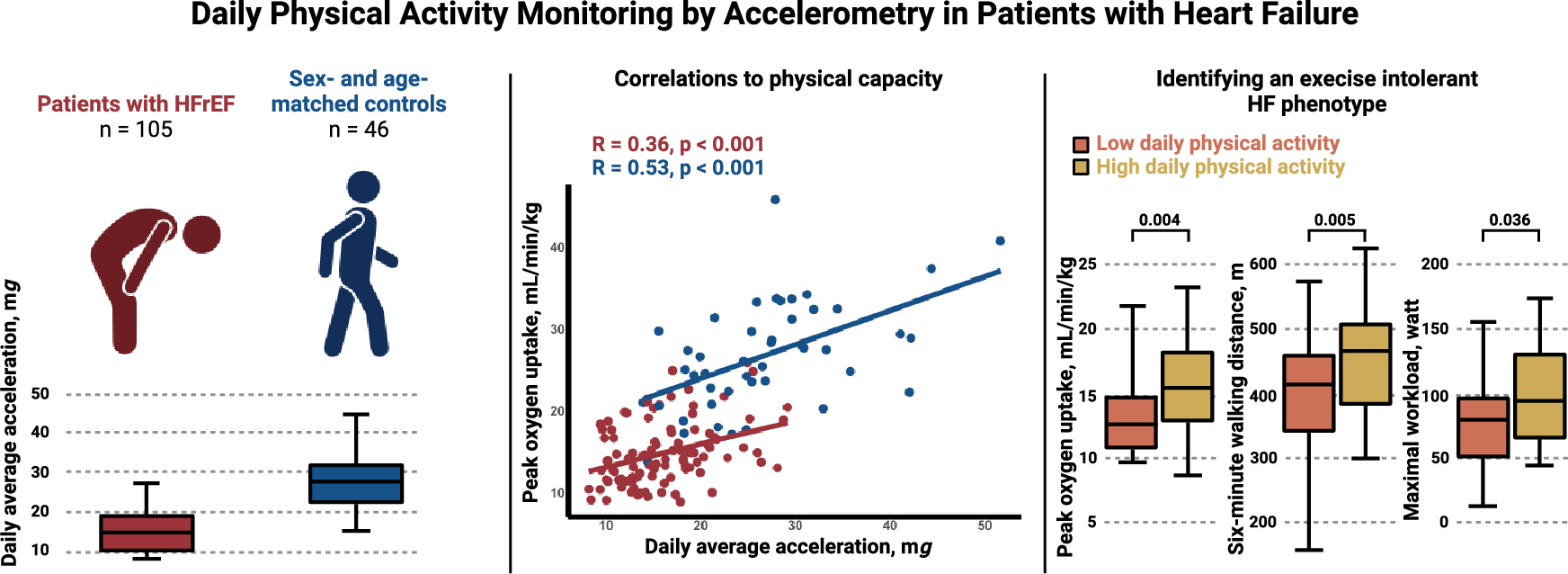
To our knowledge, this is the first study to compare daily PA between patients with HFrEF and sex- and age-matched healthy controls using accelerometry. A previous accelerometry study conducted using data from the UK Biobank showed an average acceleration of 23.7 mg in patients with HF and 28.1 mg in healthy controls [28]. The HF population was younger (66 years) and was not restricted to patients with HFrEF, which probably explains the higher average acceleration than recorded in the present study. Another UK Biobank study reported a similar average acceleration in 53 patients with HF of 21.5 mg as compared with 27.9 mg in participants without chronic diseases [23]. However, both studies were retrospective, registry-based, and lacked clinical participant data. In the present study, we support PA data with information on physical capacity, HF markers such as LVEF, NT-ProBNP, and also NYHA class, body composition, and QoL. We demonstrated a severely decreased PA level in patients with HF with a median of 12 min spent in MVPA for patients with HF compared with 56 min for healthy controls. In comparison, the World Health Organization recommends a minimum of 30 min of MVPA per day for healthy adults over 65 years of age and adults living with chronic conditions [29]. This was achieved only by 21% of the patients with HF as opposed to 89% of the healthy controls. Moreover, patients with HF spent more than 13 h daily in a sedentary state, but only 6.6 h sleeping. In contrast, healthy controls spent 10.7 h in a sedentary state and 7.3 h sleeping. Thus, our findings document that particularly time spent in MVPA and a sedentary state represent key differences between the PA of patients with HF and that of healthy controls.
Patients with HF demonstrated a higher prevalence of comorbidities and had higher BMI. Multimorbidity contributes to low PA [30], and, aside from the HF condition, the multimorbid characteristics of patients with HF may additionally reduce daily PA. As expected, healthy controls performed better on the CPET and the 6MWD test, and they exhibited higher muscle strength than patients with HF. Hence, this study demonstrated severely reduced PA and physical capacity in patients with HF.
Physical activity and known risk markers in heart failure
This study was the first to investigate correlations between objectively measured PA and well-established markers of exercise capacity in patients with HFrEF. Overall, we observed only moderate correlations. These findings have various clinical implications. CPET is the gold standard for measuring maximal exercise capacity and integrates the maximal functional capacity of the cardiac, respiratory, vascular, and musculoskeletal systems. This functional chain has numerous regulatory links from impaired cardiac function during exercise [31] and decreased skeletal muscle capillary density [32] to low peripheral oxygen extraction [33], all of which are compromised in patients with HF. The 6MWD reflects a submaximal exercise capacity under free-living conditions and may be more relevant for assessing patients’ daily life exercise capacity since they typically do not draw close to maximal effort. Both peak VO2 and 6MWD may be improved by exercise training and are known to provide strong prognostic information. We found only moderate correlations between accelerometer measurements, peak VO2, and 6MWD; and no correlations with other traditional HF prognostic markers such as LVEF or NT-ProBNP. These observations highlight that PA measurements may complement existing measures used by clinicians to assess the prognosis of patients with HF. Conversely, the only modest correlations observed between PA measurements with established HF risk markers underscore a need for more data to underpin the prognostic information of PA in patients with HFrEF.
Characterisation of patients with heart failure with low daily physical activity
As explained previously, we used average acceleration to identify a low PA group among patients with HF. Although no differences were found in age, sex, NYHA class, NT-ProBNP, LVEF, or HF duration, patients in the low PA group were characterised by a significantly lower exercise capacity than patients in the high PA group. These findings support existing knowledge of the negative association between low daily PA and exercise intolerance in HF [34]. Low PA is a well-known risk factor for the development of HF [35], and in prospective studies, it is an obvious challenge to assess daily PA in patients before HF onset. Thus, patients with HF with low daily PA may represent a low PA phenotype throughout the continuum of HF stages [36]. This low PA phenotype possibly represents a high-risk group that is poorly identified by traditional prognostic markers.
Low skeletal muscle mass was more prevalent in the low PA group: 60% of the patients were categorised as having low muscle mass compared with only 36% in the high PA group. Although skeletal muscle wasting has previously been proposed as a key marker of exercise intolerance in HF [37], we observed no differences in handgrip or knee-extensor muscle strength between the low PA group and the high PA group. A link may exist between low PA, low skeletal muscle mass, and exercise intolerance in patients with HF, but studies examining skeletal muscle wasting in patients with HF are needed to assess this issue.
Repeatability and variability of accelerometry in patients with heart failure
Accelerometry has been proposed as a novel endpoint in HF trials, but studies on accelerometry lack consistency in data collection and reporting methods. Furthermore, processing methods need to be improved as do calculating metrics based on raw acceleration [11, 38]. The present study proposes an approach to these issues by presenting average acceleration and the intensity gradient supported by time spent at various PA intensities. Repeatability in accelerometry has not previously been evaluated in patients with HF. In our study, a 12-day monitoring period showed no difference in average acceleration between weekdays and weekend days, and we reported a low day-to-day variability. Moreover, we found a low variation between the first 5 days and the last 5 days of accelerometry. The AX3 device provided raw acceleration data, which were processed in the open-source software R and RStudio using the GGIR package. This approach facilitates a high degree of transparency, reproducibility and external validation, allowing for the comparison of studies with diverse designs and settings, which was recently requested [38]. Thus, the applied accelerometer monitoring methodology proved to be robust and may serve as a framework for future accelerometry studies.
Study limitations
Only 23% of the study participants were female; a well-recognised challenge in HF trials [39]. In national registries, 30% of the incident HFrEF population is female [40]. The mean age of participants in HF clinical trials is typically approximately 65 years [41], which contrasts with the mean age (70 years) at HF onset according to data from national registries [40]. Hence, our study population, with a mean age of 72 years, matches the real-life HF population. Finally, this study was performed in stable patients with symptomatic HF in NYHA classes II and III. During recruitment, several of the patients who declined or were too frail to participate were classified as NYHA class IV. Thus, whether the results apply to asymptomatic patients or patients with more advanced HF therefore remains unknown.
Though different device positions have been used in previous daily PA studies, the wrist-worn position is the most widely applied position due to high compliance and good accuracy [19, 22]. Furthermore, the autocalibration in the GGIR package has been developed and validated with raw data from wrist-worn accelerometers [18]. Thus, we used the wrist accelerometer position to assess the study participants’ daily PA, acknowledging that other methodologies exist.
Human activity expenditure is known to be complex, and wrist-worn tri-axial accelerometry may not distinguish between types of PA (e.g. bike riding, roller-skating, etc.). Although structured exercise bouts contribute to the total amount of daily PA, most PA volume in the general population consists of walking. Our approach to daily PA reporting allows for distinction between sedentary, light, moderate, and vigorous PA. Moreover, we propose the use of the intensity gradient to describe the relative weight of intensity and volume of activity.
We used established accelerometry cutoffs for sedentary, light, and moderate PA to compare patients with HF and healthy controls. Cutoffs are debated and need to be selected carefully in different cohorts, especially in older populations. To comply with the aim of comparing patients with HF with healthy controls, we chose the most widely used cutoffs for adults.
The moderate correlations observed do not imply a direct causal relationship between accelerometer measurements and physical capacity. Multiple unmeasured factors, both physiological, psychological, and socioeconomic, may contribute to these associations. Socioeconomic factors and environmental variables, such as the walkability of areas, work locations, and access to recreational facilities, can confound or be incorrectly associated with PA levels. Seasonal variations in outdoor activities and access to exercise locations were not considered in our study, which may influence PA patterns. Psychological factors, such as motivation and perceived exertion during exercise tests, along with the inherent intra-individual variability of these tests, can significantly influence performance outcomes and contribute to the weak correlations observed. The short monitoring period for accelerometry also introduces variability. The cross-sectional design employed in our study is a limitation for obtaining complete information regarding the participants’ lifelong exercise habits and broader lifestyle factors. Such information could be relevant for understanding the influence of prior exercise routines and lifestyle choices on the daily PA patterns observed. Future research should explore these factors and apply long-term daily PA monitoring to provide a more comprehensive understanding of daily PA in diverse settings.



留言 (0)