
記住我



This study incorporates a Community-Based Participatory Research (CBPR) approach with AN/AI customer-owners, providers, and leaders to assess the acceptability and feasibility of a planned tobacco-cessation intervention [11]. CBPR is a collaborative research approach that equitably involves community members, researchers, and other stakeholders in the research process and recognizes the unique strengths that each bring.
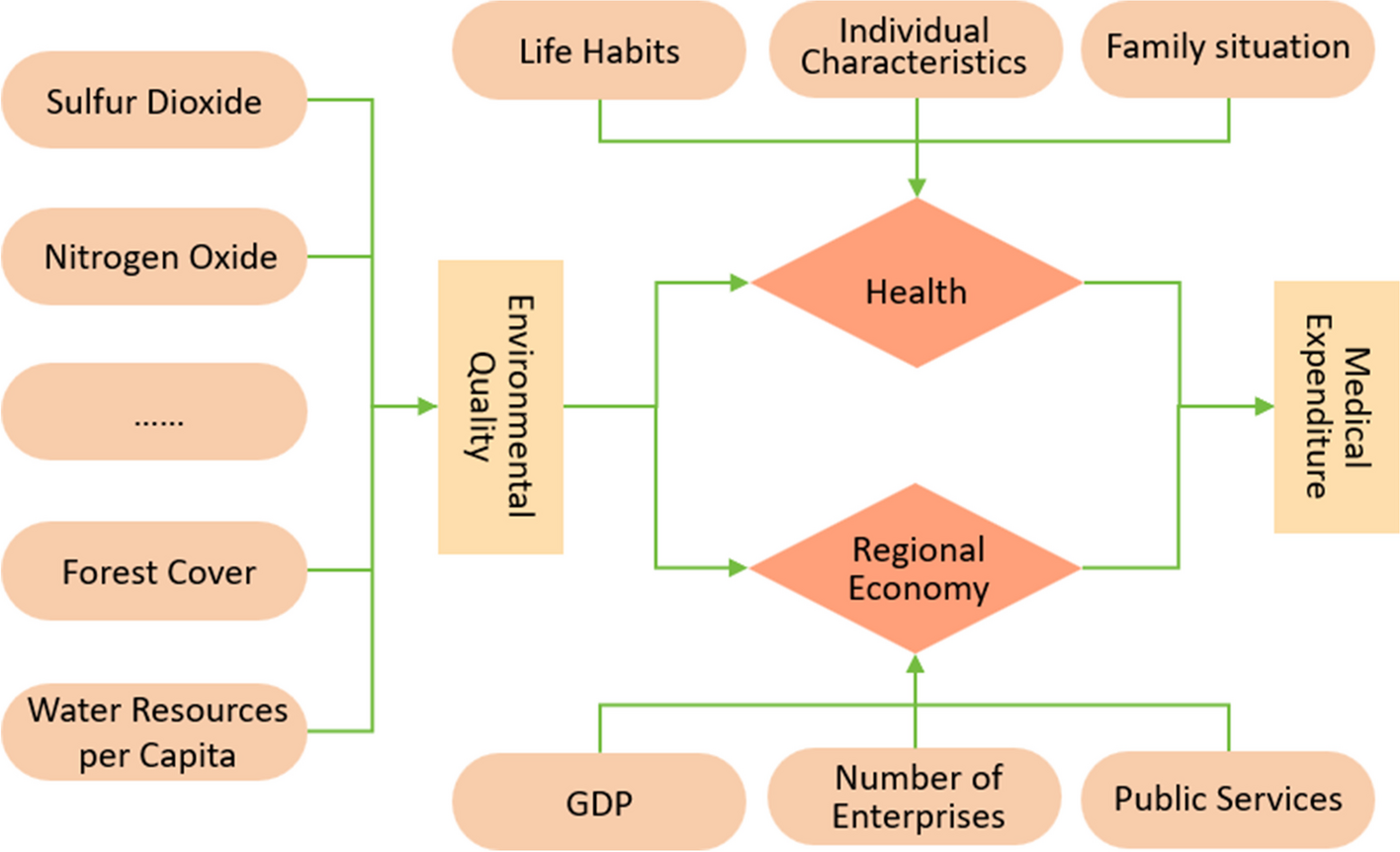
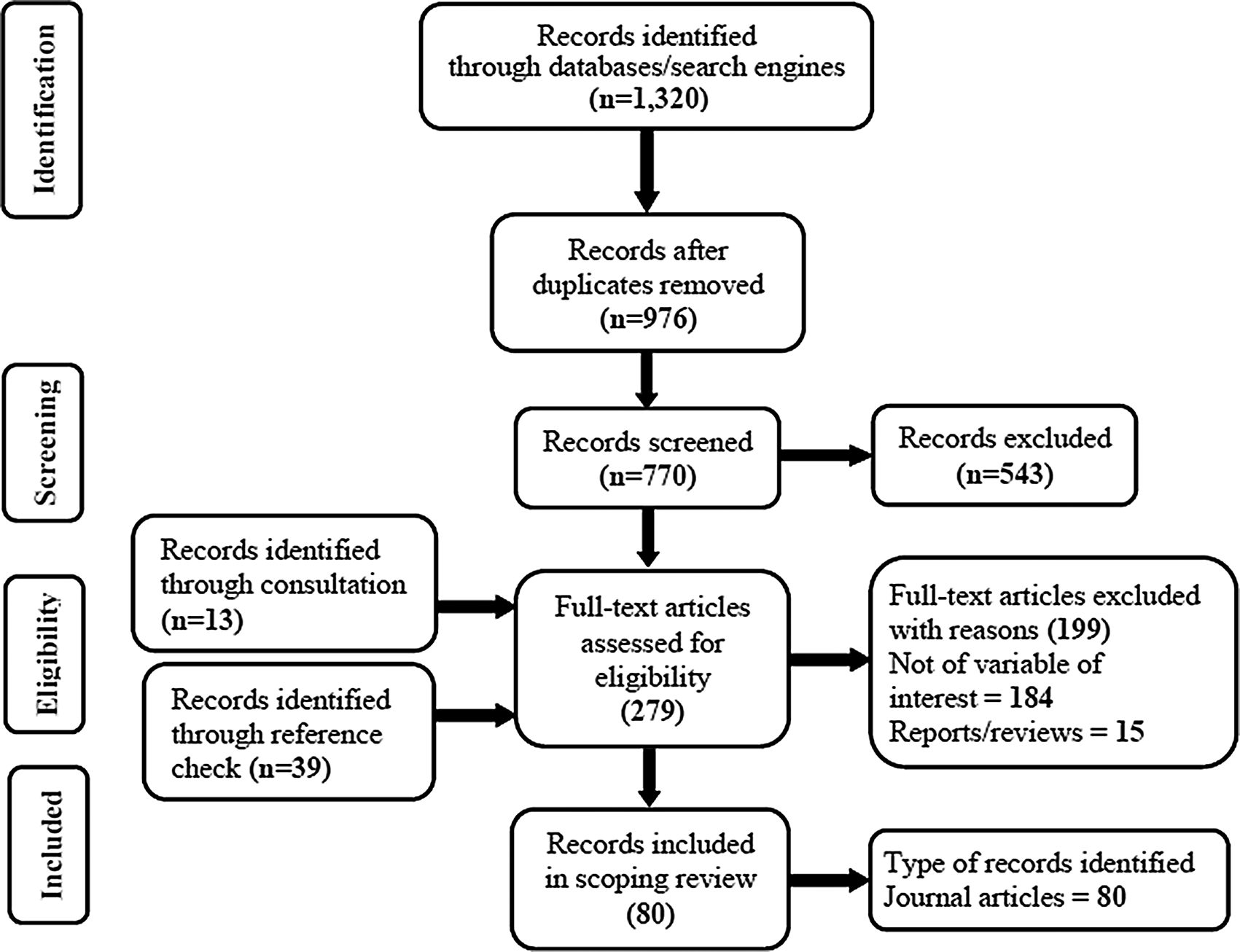
This mixed-methods study will be conducted in two phases (Fig. 1). Phase 1 is a qualitative study using individual, semi-structured interviews to elicit feedback about the acceptability and feasibility of using NMR to inform selection of pharmacologic treatment followed by a beta-test of the intervention. After refining study procedures in the beta-test, Phase 2 will pilot a single-arm trial and implementation analysis to examine factors which may impede or support implementation of the intervention within the Alaska Native Tribal health system. Our multidisciplinary team includes researchers, including AN/AI community members and persons with lived experience in quitting tobacco, with expertise in tobacco-cessation pharmacotherapy, public health, psychology, anthropology, intervention adaptation, community-engagement, and implementation science. We have also involved and appreciated AN/AI persons’ input and participation, including SCF customer-owners (i.e. SCF patients), SCF providers, and tribal health system leaders, in every phase of project development.
Fig. 1 Setting
SettingSCF serves 70,000 AN/AI peoples in the Anchorage and Matanuska-Susitna Boroughs and 55 rural villages. Most study activities will take place in SCF-owned buildings on the Alaska Native Health Campus in Anchorage, Alaska (pop. ~ 300,000). Customer-owners interested in smoking cessation typically discuss this with their primary care providers before being referred to the Quit Tobacco Program (QTP). SCF has a dedicated department within Health Education called the Quit Tobacco Program (QTP) in which customer-owners can access cessation medications, behavioral counseling, or social support to help stop smoking.
Regulatory ApprovalsOur study was approved by the Alaska Area Institutional Review Board and SCF Research Review Committee.
ParticipantsCustomer-owner participants will complete some data collection activities at home for convenience. For Phase 1, semi-structured interviews will be conducted with eligible customer owners: AN/AI persons ≥ 18 years of age who are receiving services at SCF and use cigarettes as the main form of tobacco, smoked ≥ 1 cigarette per day over the last 30 days, are willing to make a quit attempt within 30 days of enrollment in the QTP, and have phone service. Six SCF clinical/administrative leaders and six providers will also be interviewed to understand practice needs and inform intervention materials and procedures. Clinic administrators and SCF leaders known to research staff will be emailed recruitment invitations, and the list of leaders will be reviewed by the Research Oversight Committee to ensure balanced workgroup representation. An outline of the planned participant types and data collection for each is reported in Table 1.
Table 1 Participant types and data collection scheduleEligibility for Phase 2 beta-test customer owner participants will be the same as the Phase 1 interviews, plus having broadband internet connection on a mobile phone at home, work, or other location to complete smoking abstinence measures via phone or video teleconference. Interested individuals will be excluded from the beta-test if they participated in Phase 1 interviews, have participated in a smoking cessation program in the last three months, are contraindicated for the use of varenicline, have bleeding disorders, or are currently receiving cancer treatment. Care team staff eligibility for the beta-test includes being a healthcare professional at SCF and being directly involved in the care of a beta-test participant.
Eligibility for customer-owner participants in the Phase 2 pilot trial matches the beta-test; anyone who participated in an earlier phase of the study will be excluded. Phase 2 implementation interviews will be conducted with pilot trial participants, as well as SCF administrative leaders and clinical providers who have a customer-owner enrolled in the pilot trial.
To maintain a pragmatic approach to eligibility for the future trial, contraindications for NRT are not exclusionary from participation in the study. Using the current Alaska Native Medical Center Tobacco Cessation Protocol, pharmacists will not dispense medication in which participants are contraindicated and will pay special attention to any medical history precautions.
Phase 1 InterviewsSemi-structured interviews will be conducted with AN/AI customer-owners and SCF leaders and providers to refine the intervention materials and protocol. Using a sex-stratified purposive sample and based on previous sampling recommendations [15], we plan to interview approximately 36 participants to reach data saturation in the following groups: 24 customer-owner interviews (12 men, 12 women), six interviews with SCF leaders (e.g., administrators, clinical directors, tribal leaders), and six interviews with providers (e.g., primary care providers, pharmacists, tobacco treatment specialists, nurse case managers).
Separate interview guides will be developed for customer-owners and leaders/providers following the Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) implementation framework (Table 2) [16].Topics will include: (1) assessment of the needs and preferences regarding selection of tobacco-cessation medication; (2) perceived acceptability of the intervention and protocol, and procedures (communication of NMR result, timing of follow-up visits, remote vs in-person visits); (3) roles of treatment and study staff; (4) documentation process for NMR status and medication recommendation; and (5) recommendations for process and outcome measures. Interviews are expected to last up to one hour, and customer-owner interview participants will receive a $50 gift card for their time. SCF leaders and providers are paid employees and will not be compensated additionally by the study as interviews will take place during working hours. Qualitative analysis of the interview data will be used to refine the NMR-informed intervention prior to the beta-test. Qualitative data will be analyzed using ATLAS.ti.22 prior to descriptive thematic analysis.
Table 2 Application of the RE-AIM Framework to Implement Metabolism-Informed Pharmacologic Smoking Cessation TreatmentPhase 1 Beta-Test of NMR Implementation StrategyA sex-stratified, purposive sample of 10 customer-owners will be enrolled in a beta-test of the NMR implementation strategy. The goal of the beta-test will be to refine the implementation strategy before the Phase 2 pilot. Phase 1 beta participants will be recruited through SCF primary care clinics and Quit Tobacco Program (QTP) referrals, word of mouth, and study flyers. Screening will occur by phone or in-person. Confirmation of eligibility and written informed consent will occur in-person or remotely online.
Following enrollment, participants will complete a demographic survey and have a blood sample (< 5 ml) drawn prior to an intake with the QTP. Samples will be express shipped to a certified laboratory (Quest Diagnostics lab; Chantilly, VA) for NMR quantification, and results will be entered into the electronic medical record (EMR) and calculated as either slow (< 0.31) or normal (≥ 0.31) nicotine metabolism. Results are expected within 3–6 days of sample arrival at the laboratory. The appropriate therapeutic recommendation will be viewable by the care team in the EMR. Individuals with slow NMR will be recommended NRT patch. Individuals with normal metabolism will be recommended varenicline or bupropion, either alone or in combination with NRT gum or lozenge.
Although participants will be shown a list of their recommended medications, they will be able to select any of the provider-approved medications for which they are medically eligible. If an individual wishes to start medication immediately before NMR results are available, they will be recommended varenicline or bupropion (the recommendation for normal metabolizers) as NMR normal metabolizers are more common than slow metabolizers. Twelve weeks of medication will be dispensed by pharmacists through the standard clinical procedures, and participants will also have access to the usual non-pharmacologic treatments (e.g., behavioral counseling and support by phone) through the QTP. Six weeks after the participants’ quit date (set by the participant with the QTP), they will complete a follow-up survey and at-home smoking cessation tests to confirm biochemical abstinence. At-home smoking tests will be mailed to participants and will include an Ico Smokerlyzer® (Bedfont Scientific) which will connect wirelessly to their smartphone and a NicAlert™ saliva test strip which is a small and inexpensive lateral flow immunoassay test strip that is activated by eight drops of saliva. Also included in the mailed at-home test kits are step-by-step lay language instructions re-written from the original instructions. The test will also include photos of study staff self-administering both tests. Beta-test participants will receive a $50 gift card for the baseline blood draw and $75 for the follow-up study visit.
After customer-owner participants have completed the clinical process of NMR-informed medication recommendation, semi-structured interviews will be conducted with up to 20 care team members (two for each customer-owner participant). Recruitment emails will be sent to staff known to have been involved in the care of beta-test participants, and verbal consent will be obtained prior to the interview. Interviews will not be recorded, but detailed notes will be taken by the interviewer. To accommodate staff schedules, staff participants can complete a survey in place of an interview. Best-test data including demographic, acceptability questions, Electronic Health Record data and follow-up measure results will be analyzed using descriptive statistics. Content analysis will be used to analyze the interview data, brief study notes from the CO beta-test study visits and individual and group staff interviews.
Phase 2 Pilot Trial and Implementation EvaluationFollowing Phase 1, measures may be modified to reflect the results of the beta test, and a single-arm pilot trial will be conducted with 50 customer-owners to evaluate the refined implementation strategy and explore the effectiveness of the NMR for optimizing individual tobacco cessation treatment. The sample size was determined assuming a 60% retention rate to ensure at least 30 participants have follow-up data at 26 weeks [17,18,19]. Follow-up visits will be conducted as follows: at 6 weeks after starting pharmacologic treatment (to assess intervention acceptability, nicotine dependence/withdrawal, side effects, and medication adherence); at 12 weeks, the planned end of pharmacologic treatment (to assess all 6-week measures plus acceptance of study processes and biochemically verified quit status); and at 26 weeks (to assess biochemically verified quit status). Pilot-trial participants will receive the same compensation as beta-test participants for completing study procedures.
Phase 2 will also explore barriers and facilitators to implementation of the intervention within SCF to prepare for a future pragmatic trial. At the mid-point and end of the pilot trial (13 and 26 weeks), we will conduct brief, semi-structured interviews with six SCF leaders (e.g., administrators, clinical directors, tribal leaders) and six randomly selected providers who had a customer-owner who participated in the pilot trial. Interviews will assess the process of using metabolism-informed care and challenges in adhering to the treatment recommendations. Brief, semi-structured interviews will also be conducted with 12 trial participants at the mid-point and end of the pilot trial, randomly selected within sex strata, about the intervention and treatment fidelity. Trial participants will be paid $25 per interview for a total of up to $50, but SCF staff will not receive additional compensation because interviews will be conducted during paid working hours.
Outcomes and Statistical MethodsPhase 1 qualitative interviews will be thematically analyzed to inform the development of a strategy to implement NMR in tobacco cessation treatment. Quantitative and qualitative data collected in the beta-test will be used to refine study procedures in the pilot trial. The primary outcomes of the pilot trial are acceptability (Table 3) and feasibility (Table 4) of the intervention and its procedures, as assessed by study process metrics and completeness of clinical measures. Descriptive statistics will be calculated to describe sample demographics, clinical factors, tobacco history, and other co-variates. Given the nature and sample size of the single-arm pilot trial, all analyses will be treated as exploratory.
Table 3 Pilot Study Acceptability MeasuresTable 4 Pilot Study Feasibility MeasuresAcceptability and satisfaction will be assessed by calculating the mean and standard deviation of Likert-scale survey responses of items such as: timeliness and clarity of the NMR recommendation, medicine dispensation timeliness, ease of understanding trial procedures, and overall satisfaction with the intervention, compensation, and study participation. Feasibility and completeness of trial measures will be calculated based on the proportion of eligible screened participants who enroll, accrual and retention rates, proportion of enrolled participants who complete follow-up visits, proportion who use the NMR-informed pharmacologic treatment as recommended, and data completeness. Smoking abstinence at follow-up visits will also be compared to assess intervention quality and robustness. Data from this pilot trial will be used to estimate possible effect size and calculate sample size required for a future pragmatic trial.
留言 (0)