This study showed an alarming increase in the prevalence of inadequate GWG accounting for 61.2% out of 178 participants. Our findings indicate that the adequacy of GWG could be influenced by maternal factors such as pre-pregnancy BMI, educational level, adherence to the Mediterranean diet, and the average consumption of vegetables, as well as the excessive consumption of meat products. These findings may suggest the importance of promoting lifestyle interventions before and during pregnancy to ensure health and well-being for both, the mother and her infant.
No statistical significance supporting the evidence of the association between maternal age and inadequate GWG was observed. These results were inconsistent with a study conducted by Sun Y et al. [27] on a sample of 3172 pregnant women, where the authors found that an average age of 20–25 years old, is a protective factor for maintaining GWG within IOM guidelines against adverse health effects and malformations [27]. The inconsistency in findings between their results and the current study could be influenced by the huge difference in sample size of both studies. Furthermore, there was insufficient previous investigation about the effect of maternal age on GWG, which made it difficult to compare with other findings.
Current findings showed a significant association with maternal educational level, where 79% of the mothers who experienced an LGWG were holding a university degree. This result is not completely following the findings of a previous systematic review of observational studies that was conducted by O’Brien et al. [17], where pregnant women with low educational levels were less likely to maintain GWG within IOM recommendations. Further investigations must be performed on a larger sample targeting highly educated mothers to identify if their level of awareness about not gaining weight in excess during pregnancy, is negatively transformed into a GWG less than the recommendations.
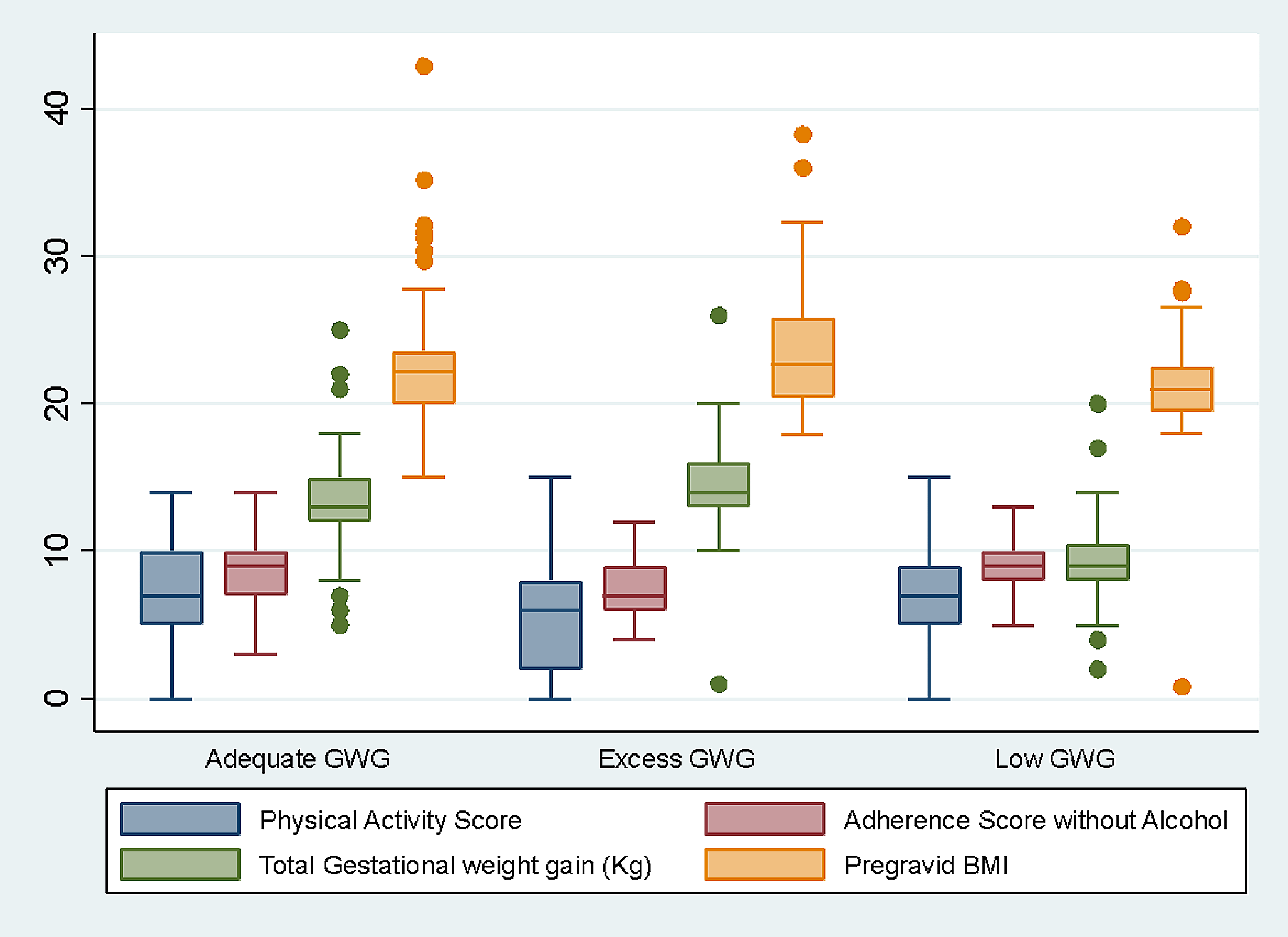
Concerning pre-pregnancy BMI, our findings suggested a statistically significant association with GWG, as participants with pre-pregnancy overweight or obesity were more likely to experience EGWG, increasing the risk of adverse health consequences for the mother and her infant. This finding was consistent with previous studies, where women with a pre-pregnancy BMI value ≥ 25 Kg/m2, experienced EGWG and were at higher risk of developing GDM and/or pre-eclampsia, having preterm or cesarean birth, hemorrhage, infection and many other complications [1, 8]. EGWG has been reported with an increased likelihood to retain weight after delivery, which is usually followed by a higher possibility of developing postpartum obesity and suffering from other difficulties during future pregnancies, as well as giving birth to large-for-gestational-age infants, who will also be at higher risk to develop childhood overweight or obesity and its associated consequences [7, 9]. However, it was not possible to comment on the outcomes of our findings as this data was not yet collected.
In the present study, the adherence to the MD was significantly associated with GWG in comparison with IOM guidelines [1, 2], suggesting a potential benefit for the health of both, the mother and her infant. Participants with low adherence were more likely to experience EGWG. These results were in line with previous studies where lower GWG was associated with higher adherence to the MD before and during pregnancy [28,29,30]. In another systematic review, some of the selected studies highlighted the importance of MD during pregnancy to prevent excessive GWG, while others confirmed its association with a decreased risk of maternal and fetal complications [19]. This alignment with the existing literature confirms the importance of dietary interventions in the management of GWG and prevention of its adverse health consequences. Moreover, for a better understanding of this association, it is highly recommended to create or validate a questionnaire that is suitable for this population to detect adherence. Although our study did not measure the impact of MD adherence on newborns, the association with GWG suggests potential implications on the health of the infants and children. Previous studies also showed association between adherence to the MD and reduction of some pregnancy and childbirth complications as well as perinatal and childhood problems [19].
In terms of physical activity score, our findings imply no association with GWG, where score differences between GWG categories were relatively small, but higher among AGWG and LGWG indicating that more active pregnant women were less likely to gain excessive weight during pregnancy. This finding was in accordance with the systematic review results of O’Brien et al. [17] where PA was shown to be significantly inversely associated with GWG. It was also proposed by Teede et al. [14], that PA-based interventions are associated with reduced GWG as well as maternal and neonatal health risks. However, the highest mean value of PA score in our results was detected among the LGWG category, and this could also be linked to the high educational level of our participants. Perhaps, they tend to be more active due to their awareness of the importance of PA during pregnancy, leading to insufficient GWG. In 2019, O’Brien et al. [12] conducted a data meta-analysis about the impact of maternal education on GWG, indicating an increased risk of inadequate GWG among highly educated mothers following a mixed intervention of diet and PA-based interventions. Further investigations needed to be performed on a larger sample size, taking into consideration this relationship between educational level and physical activity and their association with GWG especially in terms of LGWG.
Maternal smoking habits were not associated with GWG. In contrast to our findings, a previously conducted systematic review by Zhou et al. [16], showed that smoking during pregnancy was associated with EGWG. However, our results may be influenced by the fact that only 6 participants from the whole sample were smokers, and those were equally distributed between AGWG and EGWG categories. Further examination is needed on a larger sample size.
Regarding the average daily consumption of vegetables that was shown in our study, to be associated with a lower risk of EGWG, our suggestion for future investigation is to identify if there is a link between high levels of maternal education and adequate consumption of vegetables on a larger sample size. This result could be considered following a previously conducted cohort study by Hirko et al. [31], where women with obesity who consumed more fruits and vegetables during pregnancy, were less likely to experience EGWG [31].
As for the excessive daily consumption of red meat, a significant association was detected with an increased risk of EGWG. A study conducted by Maugeri et al. [32], showed an increase in the trend of EGWG that was linked to the consumption of western dietary pattern, which means a high consumption of red meat and fast-food products [32].
Our study encompasses some limitations. The sample size is considered small, which may hinder the detection or be the reason for some associations and therefore affect the statistical power of the study. For this reason, we recommend future investigations incorporating larger sample sizes to better explore these associations. Unfortunately, we did not include other potential factors that could influence GWG such as “income”, since we did not collect this data, and “employment status” as there was a significant number of missing responses from our study participants. Additionally, pre-pregnancy weight and total GWG were self-reported by the participants and not measured by the trained dietitians, which increases the potential risk for bias by reducing the overall reliability of the data. Moreover, the lack of availability of a valid tool for assessing the adherence to the MD that is tailored to pregnant women, is a major limitation, as we had to adapt an existing questionnaire by removing the item of “alcohol consumption” and reducing the score, which affects its validity. Future research should focus on developing an assessment tool that is tailored to this specific population to enhance the robustness of the dietary assessment. However, this could also be considered as a strength of our study as we tried to make the measurement tool more relevant to our population to obtain meaningful data, as well as addressed a gap in the existing literature which is the absence of a valid questionnaire that measures adherence of the MD in pregnant women, taking into consideration the international guidelines in pregnancy which state the importance of avoiding alcohol within this critical period. Another key strength is the use of a section from the previously validated questionnaire by Turconi et al [25]. to assess PA levels among participants. Last but not least, our study provides a new region-specific data on GWG adequacy and its associated factors in the Lombardy region, offering insights to the policymakers and healthcare providers to develop new health interventions at the local level.
This study affirmed conclusions from previous research on the association between lifestyle factors including the adherence to the MD, before and during pregnancy, and the maintenance of GWG within IOM guidelines. An alarming increase in the rate of pregnant women with inadequate GWG was revealed, indicating a significant association with maternal educational level, pre-pregnancy BMI, adherence to the MD, average daily consumption of vegetables, and excessive consumption of meat products. The small sample size imposes a major limitation on our findings, however, the absence of a valid questionnaire that could assess MD adherence in pregnant women was detected as a gap in the literature and emphasized the importance of future research to fill it. Our results emphasize the importance of promoting lifestyle interventions during childbearing age as well as during pregnancy, as a crucial public health strategy to ensure health and well-being for two of the vulnerable groups, pregnant women, and infants.






留言 (0)