
記住我








A 71-year-old man underwent catheter ablation for AF 4 years earlier. During follow-up, there were no indications of a patent foramen ovale or an iASD, nor were any other intracardiac shunts detected during subsequent TEE (Fig. 1). He was hospitalized for recurrent AF and heart failure symptoms, including palpitations and fatigue. On admission, transthoracic echocardiography (TTE) showed a mildly reduced ejection fraction of 41%, without significant valvular abnormalities or intracardiac shunts. While receiving inpatient treatment for heart failure, the patient suddenly reported abdominal pain, which was followed by cardiac arrest. Immediate life-saving measures, including chest compressions, tracheal intubation, and administration of epinephrine, restored spontaneous circulation.
Fig. 1
In the transesophageal echocardiogram taken within 3 months after catheter ablation treatment, there was no evidence of a patent foramen ovale or an iatrogenic ASD, nor were any other intracardiac shunts. The image shows the superior and inferior vena cava of the middle esophagus
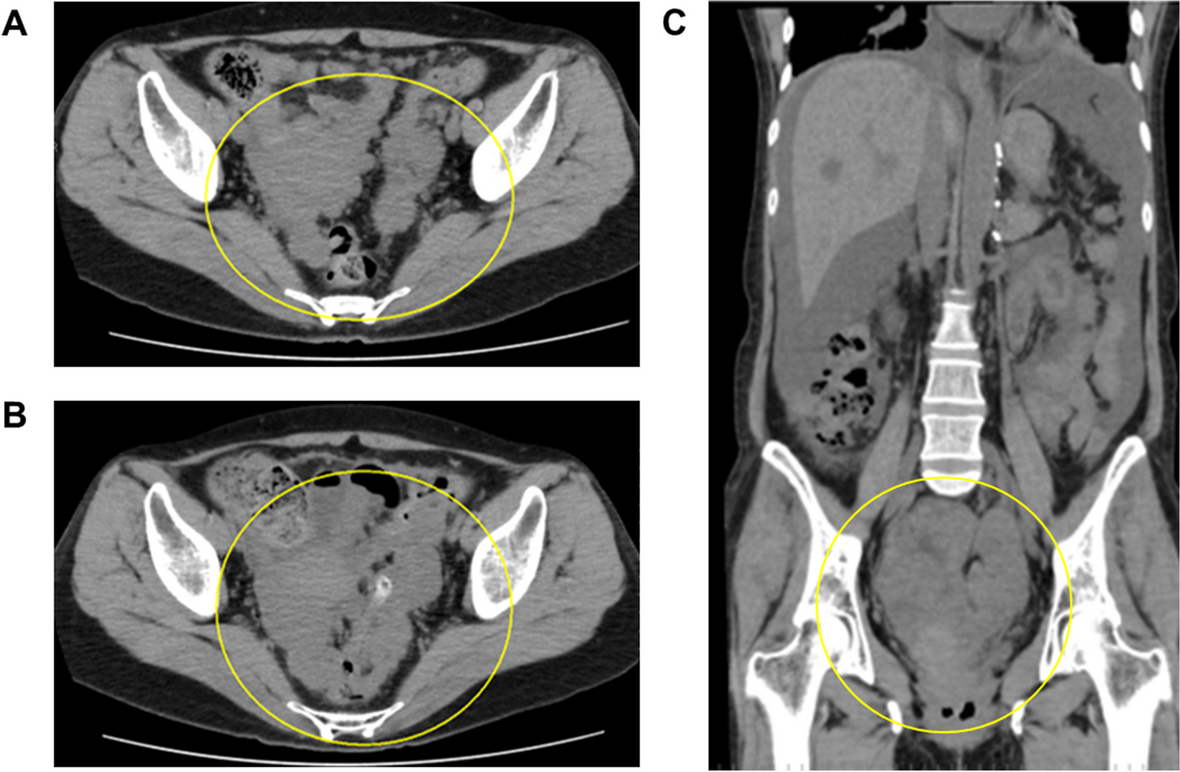
Contrast-enhanced computed tomography (CT) of the chest and abdomen revealed a rupture of the AAA into the IVC (Fig. 2). No intracardiac shunts were identified on CT. Due to limited space near the renal arteries, endovascular stent graft placement was deemed inappropriate, necessitating emergency open abdominal aortic replacement surgery.
Fig. 2
On contrast-enhanced computed tomography, an aorto-caval fistula that occurred due to the rupture of an abdominal aortic aneurysm was identified
Before surgery, the patient had a blood pressure of 100/50 mmHg with continuous norepinephrine infusion at 0.2 μg/kg/min, a central venous pressure (CVP) of 35 mmHg, a pulmonary artery pressure (PAP) of 43/37 mmHg, an irregular pulse rate of 120 beats/min (AF), oxygen saturation of 97% (FiO2 1.0), and a body temperature of 35.0 °C. The patient’s hemoglobin level was 13.2 g/dL upon admission but decreased to 10.6 g/dL at the start of surgery. On TTE, cardiac contractility had remained unchanged, but signs of increased right heart strain were observed.
General anesthesia was planned. The airway was secured through endotracheal intubation, and central venous access was established during resuscitation. Standard monitoring along with arterial blood pressure (ABP), CVP, PAP, electroencephalogram (BIS®), cerebral oximeter (INVOS®), and neuromuscular transmission (TOF-Watch®) was utilized. We monitored bladder temperature and maintained the body temperature using a warming device (Bair Hugger®). Cerebral oxygen saturation upon arrival in the operating room was approximately 50% bilaterally. Anesthetic induction was initiated using 1% sevoflurane, 100 μg of fentanyl, and 50 mg of rocuronium. Anesthesia was maintained using sevoflurane, rocuronium boluses, and fentanyl boluses. Immediately when surgery was started, substantial venous bleeding was observed from various sites, including the incision site. We used the Belmont® Rapid Infuser System to administer fluids and blood transfusions at a maximum rate of 500 mL/min for managing large-volume fluid needs.
Despite massive blood transfusions, continuous norepinephrine infusion at 0.2 μg /kg/min, and repeated bolus epinephrine of 30–40 μg, ABP decreased to 50/20 mmHg with persistent increase of CVP to 35 mmHg. The hemoglobin level reached its lowest point of 7.2 g/dL. Cerebral oxygen saturation decreased to 20%. TEE revealed a right-to-left shunt through the central foramen ovale with a peak pressure gradient of 16 mmHg, while both left and right ventricular systolic function remained unchanged (Fig. 3, Supplementary Video). An intra-aortic balloon occlusion (IABO) was inserted in the descending thoracic aorta from the femoral artery and immediately resulted in an increase of ABP to 140/50 mmHg with a decreased of CVP to 10 mmHg and PAP to 25/10 mmHg. Cerebral oxygen saturation increased to 50–60%. TEE revealed disappearance of right-to-left shunt (Fig. 4), and venous bleeding was controlled. However, arterial bleeding persisted, and fibrinogen level was 89 mg/dL, necessitating transfusion of fresh-frozen plasma and fibrinogen concentrate of 6 g before successful surgical hemostasis. The surgery proceeded well, closing the fistula with a patch, and replacing the abdominal aorta with a Y-shaped artificial graft. The surgery lasted 339 min with an estimated blood loss which was 21,557 mL. Transfusions included 3360 mL of packed red blood cells, 7200 mL of fresh-frozen plasma, 600 mL of platelet concentrate, and 8120 mL of autologous salvaged blood (Fig. 5). At the end of the surgery, the hemoglobin level had increased to 10.5 g/dL, and fibrinogen levels had risen to 210 mg/dL. Due to significant bleeding and massive transfusion, the body temperature dropped to 34.0 °C. In the ICU, the patient underwent warming, resulting in a return to approximately 36.0 °C within 4 h. Bilateral pleural effusions and significant edema were identified postoperatively, taking time to resolve. Extubation was performed on the 6th postoperative day, and the patient was discharged home without other complications on day 30.
Fig. 3
A Intraoperative transesophageal echocardiography showed a right-to-left shunt through the foramen ovale. B The peak pressure gradient was 16 mmHg
Fig. 4
After intra-aortic balloon occlusion (IABO), the right-to-left shunt at the central part of the foramen ovale was no longer detectable
Fig. 5
Anesthesia record. TEE, transesophageal echocardiography; X, start and end of anesthesia; ◎start and end of surgery; SpO2, saturation of percutaneous oxygen; ABP, arterial blood pressure; PAP, pulmonary artery pressure; CVP, central venous pressure
留言 (0)