
記住我
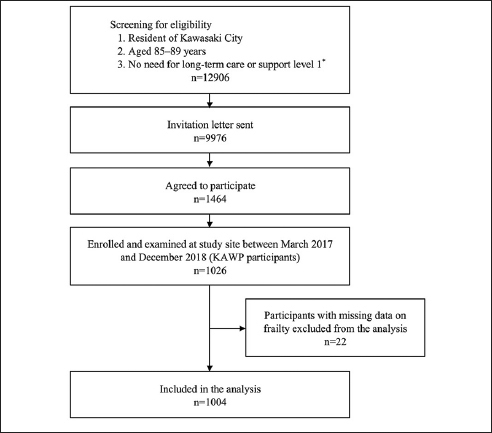








We included all patients aged 65 years or more, who had at least one admission to one of our five acute public hospitals across the South Western Sydney (SWSLHD) Local Health District between January 1st 2010 and December 31st 2020. Our analysis is based on the first (index) admission during this period. We have included both unplanned (emergency) and planned admissions, with at least an overnight stay in the hospital, excluding day-only admissions such as those for renal replacement therapy and ambulatory care.
Estimating frailty status on admission to hospitalFrailty among these older patients was estimated using a cumulative deficit approach developed by Clegg et al (9), using clinical coding (ICD-10-codes) of 36 deficit items (Appendix 1). We have found locally that this approach to estimating frailty performs well in predicting mortality (c-statistic = 0.70), and inspection of survival curves from our hospital population are comparable to those from Clegg’s population-based development model, in which increasing deficit items groups are related to increased mortality (9). We have also previously shown that this cumulative deficit approach using coded hospital data, performs comparably to Rockwood’s Clinical Frailty Scale in predicting an acute episode of delirium in the adult intensive care setting (both c-statistics = 0.70) (10). In our cohort, cumulative deficit items were identified from pre-existing conditions at the time of hospital admission. These were coded as part of routine hospital administrative data collection. Specifically, four cumulative frailty item groups were derived based on the distribution of items: 0–1 item; 2 items; 3 items; and 4–13 items. Grouping is based on using the lower and upper 99th population percentile of deficit items (in our case 0 and 4). This range is divided into four equally distanced groups as suggested by Clegg et al (9). Using this approach the two highest deficit items groups are considered moderately and severely frail, respectively. Using this criterion we have used 3 or more deficit items to indicate the presence of frailty on admission to the hospital. Rather than using an index we present the actual number of items. The distribution of the deficit items in our cohort is presented in Figure 2.
Figure 2
Distribution of cumulative deficit items
AF = atrial fibrillation, IHD = ischaemic heart disease, CKD = chronic kidney disease, CVD = cardiovascular disease, and PVD = peripheral vascular disease.
Outcomes of interestOur main outcomes of interest were based on Hospital Acquired Complications (HACs): (1) falls; (2) pressure injury; (3) delirium (4); malnutrition; and (5) thromboembolism. And Hospital Acquired Infections (HAI): (1) multi-resistant organisms (MRO); blood-stream infections (BSI); surgical site infections (SSI); catheter-associated urinary tract infections (CAUTI); and acute pneumonia (AP). All these complications are routinely identified and coded as part of our national hospital coding standards, using ICD-10-AM codes and specifically identified as being hospital-acquired by an associated hospital-onset flag code (11).
Statistical analysisThe characteristics of the cohort of older adults admitted to our hospitals are presented using descriptive statistics, and the number of adverse events are presented as rates with associated 95% confidence intervals (95% CI), per 1000 admissions. The association between an increasing number of frailty deficit items and the risk of specific hospital-acquired adverse events (HAC, HAI) was assessed using Poisson regression, adjusted for age and sex. Estimates are presented as Rate Ratios (RR) and associated 95% CI (12). The numbers of cumulative frailty deficit items are presented in four groups (0–1 item, 2 items, 3 items, and 4–13 items). The population-attributable risks of any HAC or HAI, based on the proportion of frail older adults (3 or more deficit items, as suggested by Clegg et al (9)) were also estimated (8, 13).
$$\text=(\mathrm(\text-1))/(\mathrm(\text-1)+1)$$
Where, popAR = population-attributable risk, p = the proportion of exposure among the given population (in our case the proportion of older adults with 3 or more deficit items), and RR = adjusted (age and sex) Risk Ratio. The adjusted model areas under the receiver operator characteristic curves and associated 95% CI are presented (AUC). The absolute risk of these adverse events during a hospital stay based on age, sex, and the number of cumulative deficit frailty items groups are presented, with 95% CI. All data management was undertaken using SAS (version 9.4), and all statistical analyses were performed using the R language for statistical computing (14).
Ethical ConsiderationsThis project was reviewed by the SWSLHD Local Health District Human Research Ethics Committee and was determined to meet the requirements of the National Statement on Ethical Conduct in Human Research (2007). Due to the use of routinely collected hospital separation data, the need for individual patient consent was waived (HREC code – ETH11883).
留言 (0)