
記住我






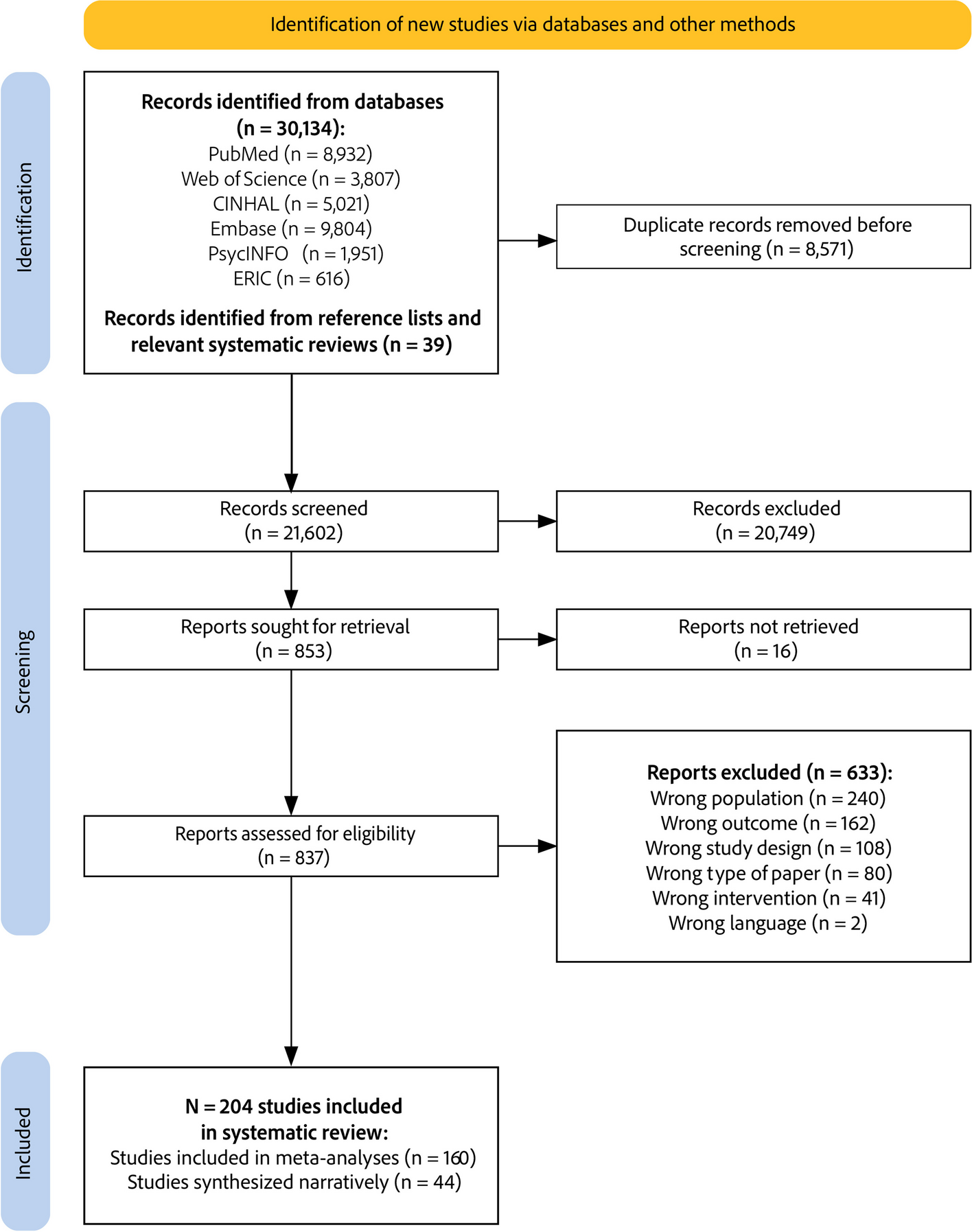
We identified 2631 records after de-duplication stemming from the database search (n = 2603) and searches of other sources (n = 28). After abstract screening, we assessed 277 full texts and identified 109 SRs (110 articles) meeting our predefined eligibility criteria. We excluded 54 (55 articles) after evaluating their quality as having critically low confidence in their reported results. A description of the excluded SRs is listed in Additional file 1, eTable 5 and eTable 6. To minimise overlap in the included SRs, we did not extract data from a SR if the included primary studies were also included in other SRs (n = 3) or if other included SRs provided more up-to-date information (n = 5) (Additional file 1, eTable 7). Further SRs did not exactly address the same research question applying the same eligibility criteria. Finally, we included 46 SRs for data synthesis and analysis. Figure 1 shows the details of the study selection process, and Table 2 provides an overview of the included SRs.
Table 2 Overview of included SRsFig. 1 SR characteristics
SR characteristicsThe 46 included SRs spanned seven distinct healthcare practices: ‘Drug treatments: antibiotics’ (n = 20), ‘Laboratory tests’ (n = 5), ‘Drug treatments: opioids’ (n = 4), ‘Diagnostic imaging’ (n = 4), ‘Drug treatments: antipsychotics, benzodiazepines’ (n = 3), ‘Mixed diagnostic tests’ (n = 3), and ‘Other interventions’ (e.g. utilisation of caesarean sections, central venous catheters [CVCs] or stress ulcer prophylaxis pharmacotherapy, n = 7) (see Fig. 2). Among the 46 SRs, 32 synthesised the results narratively; 14 provided at least one MA result. The confidence levels in the SR results varied, with the majority rated as low confidence (n = 22), followed by moderate (n = 17) and high confidence (n = 7). The major reasons for downgrading were: no statement that an a-priori protocol existed (n = 12), and the SR did not account for the included primary studies’ RoB when interpreting the results. For a more detailed description, see Additional File 1, eTable3. SRs with high confidence ratings were predominantly found in the ‘Drug treatments: antibiotics’ category (n = 6). The certainty of evidence was assessed in seven SRs. The GRADE ratings of the selected outcomes and SRs are listed in Additional File 3.
Fig. 2
Confidence assessments of the included SRs (see also reference [73] to explore the online figure)
The primary studies included in the SRs were published between 1974 and 2022. The most extensive timeframe is observed in the ‘Laboratory tests’ category, covering 47 years (1974–2021), followed closely by the ‘Drug treatments: antibiotics’ category, ranging 46 years (1976–2022). The number of included primary studies in the SRs ranged from two to 221 (see Additional File 1_eTable8).
The included SRs encompassed a variety of settings; most focused on secondary/tertiary care (n = 17) (see Table 3). The primary care setting was prevalent in ‘Drug treatments: antibiotics’ (11/12 SRs). Among all the SRs, family medicine was the most frequently represented medical field (n = 10). The ‘Other interventions’ category contained SRs addressing multiple specialties or SRs with missing information (n = 22). Approximately 50% of the included primary studies were conducted in North America and 26% in Europe, with variations across healthcare practices. The primary de-implementation rationale was ‘Evidence suggests more harms than benefits for the patient or community’ (n = 36). The SRs described the study aims primarily as ‘reducing LVC’ (n = 43) (see Additional File 1_eTable 9).
Table 3 Characteristics of the included SRsDe-implementation initiative characteristicsTaxonomies for categorising de-implementation strategies were seldom applied. The EPOC system was most often used (n = 6) [7, 13], followed by Michie et al.’s [8, 12] intervention functions (n = 1) and a combination of both taxonomies (n = 3). Further, 14 SRs did not apply a taxonomy but specified the investigated de-implementation strategies via the inclusion criteria (e.g. SR focused on ‘audit and provide feedback’). Two SRs used additional tools to categorise de-implementation strategies (see Additional File 1_eTable 10).
Figure 3 depicts the frequency of ERIC strategy clusters resulting from our coding of the strategies included in the SRs. Strategies related to the train and educate stakeholders cluster were applied at least once in individual studies in 41 SRs. Other frequently applied strategies reflected the support clinicians, use evaluative and iterative strategies, and change infrastructure and workflow clusters. Notably, the individual SRs examined between one and seven ERIC strategy clusters (median = 4). We identified a category not previously mentioned in the ERIC compilation. Changes in scope and nature of benefits and services was used to describe offering dementia patients physical or social exercises to reduce antipsychotics or offering the general population physical therapy to reduce opioid consumption. The ERIC strategy clusters were employed with similar frequency across different healthcare practices (Additional File 1_eFigure 1).
Fig. 3
ERIC strategy clusters addressed in SRs (n = 46)
The included SRs seldomly reported details on de-implementation initiatives. Information on temporality (i.e. when was the de-implementation initiative target group addressed) and on duration or intensity (i.e. dosage) was provided in ten and seven SRs, respectively. The initiatives’ development was addressed in one SR, detailing whether the included primary studies reported using guidelines for initiative design and implementation. None of the SRs provided information about tailoring use (i.e. choosing de-implementation strategies based on a contextual assessment of barriers and facilitators). While all SRs reported healthcare providers as the targets of de-implementation initiatives, 13 additionally named patients as targets (see Additional File 1_eTable 11).
Participant detailsThe patient population in the included SRs ranged from 1,595 to 2,529,855. Details on age and participants’ (patients or health professionals) gender were often not reported. The observation period ranged from four days to 17 years. Long-term outcomes (> 12 months) were reported in only six SRs (see Additional File 1_eTable 12).
Effectiveness of de-implementation initiatives according to healthcare practicesDrug treatment: antibioticsWe identified 20 SRs investigating the effectiveness of de-implementation initiatives aimed at curtailing antibiotic utilisation; four also reported on the reduction of inappropriate antibiotic prescriptions [28, 31, 38, 42]. Our assessment categorised six of the included SRs as having high confidence in the results [28, 30, 34, 35, 39, 44], six as moderate confidence [27, 37, 38, 41, 43, 45], and eight as low confidence [29, 31,32,33, 36, 40, 42, 46]. Overall, 11 SRs reported statistically significant positive reductions in antibiotic utilisation [27, 28, 32,33,34,35, 37, 39,40,41, 43]. Five of these studies reported on the certainty of evidence using the GRADE assessment ranging from very low [43], low [27, 39], moderate [27, 39, 43, 44] to high certainty [28] of the evidence For example, a MA of a high-confidence Cochrane review [28] showed a reduction of 1.95 days in antibiotic treatment durations (95% confidence interval [CI]: 2.22 to 1.67; 14 randomised controlled trials [RCTs], high level of certainty). Additionally, six SRs showed inconsistently positive reductions in antibiotic utilisation [29, 36, 42, 44,45,46], while the remaining three [30, 31, 38] found no statistically significant change in ≥ 50% of the included primary studies) (see Fig. 4). Outcomes pertaining to the appropriateness of antibiotic prescriptions were less frequently explored. Two SRs reported statistically significant positive results [28, 42], and two indicated no change in the appropriateness of antibiotic prescriptions [31, 38].
Fig. 4
Harvest plot for LVC utilisation and appropriateness (nSR=46)
Explanation figure: This harvest plot represents the ‘low-value care use (utilisation)’ and ‘appropriateness of care use’ outcomes. Each included SR is represented as a bar in the matrix at least once and twice if the SR reported on both outcomes
Bar position: (see Table 2): Row ‘positive’ (< 75% or MA showing an effect), ‘inconsistent positive’ (< 50–75%), or ‘no change’ (≥ 50% or MA showing no effect)
Bar colour: Healthcare practice (see legend)
Bar height: Confidence in the results according to the AMSTAR 2 assessment
Number above the bar: Number of included primary studies in the SR
Lowercase “u” under a bar: Relevant information for assessing the primary studies’ statistical significance was not reported in the SRs
Thirteen SRs provided data regarding the effectiveness of seven distinct ERIC strategy clusters, presented in detail below [27, 29, 30, 32,33,34,35,36,37, 39, 43,44,45].
Change infrastructure and workflowThis cluster comprised two discrete de-implementation strategies: delayed versus immediate prescription categorised in ‘assess and redesign workflow’ and the application of point-of-care tests categorised in ‘change physical structure and equipment’. Two MAs showed a reduction in antibiotic utilisation for respiratory infections for delayed versus immediate prescriptions (odds ratio [OR]: 0.04, 95% CI: 0.03 to 0.05 [44] and OR: 0.09, 95% CI: 0.03 to 0.23, respectively [35]). This effect diminished when delayed prescription was compared to no antibiotics [44]. The application of different point-of-care tests, such as the c-reactive protein and procalcitonin test, reduced antibiotic utilisation in URTI treatment in two MAs (c-reactive protein: risk ratio [RR]: 0.79, 95% CI: 0.70 to 0.90, 13 RCTs [39] and RR: 0.77, 95% CI: 0.69 to 0.86, 12 RCTs, and procalcitonin measurements: RR: 0.32, 95% CI: 0.23 to 0.44, 1 RCT) [35] and in one SR’s narrative synthesis [29]. Supplementary tests, including nasopharyngeal swabs, contributed to a non-statistically significant reduction in prescribed antibiotics (RR: 0.89, 95% CI: 0.71 to 1.12) [
留言 (0)