
記住我



Obesity is a major public health concern worldwide, with a growing number of individuals affected. Despite the availability of various weight loss interventions, many individuals struggle to achieve and maintain a healthy weight. One treatment for obesity is AS, which has been shown in clinical trials to be effective in reducing stress and anxiety (Usichenko et al., 2022). Embedded ear needles were popularized in the ‘70s and ‘80s for weight loss (Schatz, 1975), which might have propagated the conduct of many clinical trials using auricular therapy for various conditions (insomnia, cocaine addiction, back pain, and epilepsy; Gates et al., 2006; Lan et al., 2015; Liu et al., 2018; Moura et al., 2019; Mendonça et al., 2020; Yap et al., 2020). Currently, it is presumed that AS exerts its effects through the involvement of cranial nerves V, VII, and X, which lead to the modulation of brain areas involved in stress response, such as the limbic system, locus coeruleus, and hypothalamus (Qu et al., 2014; Frangos et al., 2015). The main response is seen in connection to the vagal nerve, which presents on the auricle (Arnold’s nerve) and can be directly stimulated in the cymba and the region around the meatus acusticus externus (Peuker and Filler, 2002; Peuker, 2003). This study aimed to provide a comprehensive and systematic review of RCTs assessing the effects of AS on weight reduction and obesity-related parameters such as waist circumference, waist-to-hip ratio, and blood lipids in obese patients. The study aimed to provide a better understanding of the potential benefits and limitations of AS as a treatment strategy for weight loss in obesity and its effect on obesity-related parameters.
1.2 ObjectivesSystematic review and meta-analysis to evaluate the effects of AS on obesity-related parameters and the safety of AS.
2 MethodsThe systematic review protocol has been registered on PROSPERO ID CRD42020184795. The systematic review and meta-analysis were conducted in accordance with the Cochrane Handbook for Systematic Reviews of Interventions and the PRISMA guidelines. The protocol aimed at an investigation of the effects of AS on a large array of biomarkers and other objective outcomes. This study focuses on obesity-related outcomes.
2.1 Eligibility criteria for included trials in the review 2.1.1 Types of trialsOnly RCTs with a full text published in European languages were eligible for the review.
2.1.2 Types of participantsObese patients have no restrictions on age, sex, ethnicity, or further health conditions. Obesity was defined as a BMI greater than 25 (Engin, 2017). If other ethnic groups are investigated, adjusted BMI will be applied. For Asian Americans, the adjusted BMI for obesity is defined as a BMI greater than 23 (Jih et al., 2014).
2.1.3 Types of interventionsWe included all RCTs in which AS was used alone or in addition to further weight loss measures. All interventions were eligible, including traditional AS (i.e., auricular acupuncture, auricular acupuncture with electric stimulation, and auricular acupressure) as well as related techniques such as transcutaneous electrical stimulation of the auricular nerve (tVNS) [synonym: transauricular vagus nerve stimulation (taVNS)] or cranial electrotherapeutic stimulation (CES, on the ear lobule). All control conditions (sham or placebo stimulation, diets, exercise, routine care, etc.) were included. We excluded studies that compared one type of AS technique only with another AS technique.
2.1.4 Types of outcome measuresThe main outcomes were body weight and BMI, body fat, waist circumference, hip circumference, waist/hip circumference ratio, blood lipids, cholesterol, and obesity-related blood chemistry (HbA1c, blood glucose, leptin, ghrelin, and homeostasis model assessment index). All biomarkers, that were reported with results were extracted and evaluated. The continuous data were pooled in a meta-analysis, while the non-continuous data were evaluated descriptively. Adverse event reporting was used to analyze safety.
2.2 Search methods for identification of trials 2.2.1 Electronic searchesTwo researchers (JD and KH) searched the following databases from inception until 17 November 2021: MEDLINE (PubMed), EMBASE, Cochrane Central Register of Controlled Trials (CENTRAL), ISI Web of Science, and Scopus Database. The complete search strategy is listed in Table 1.
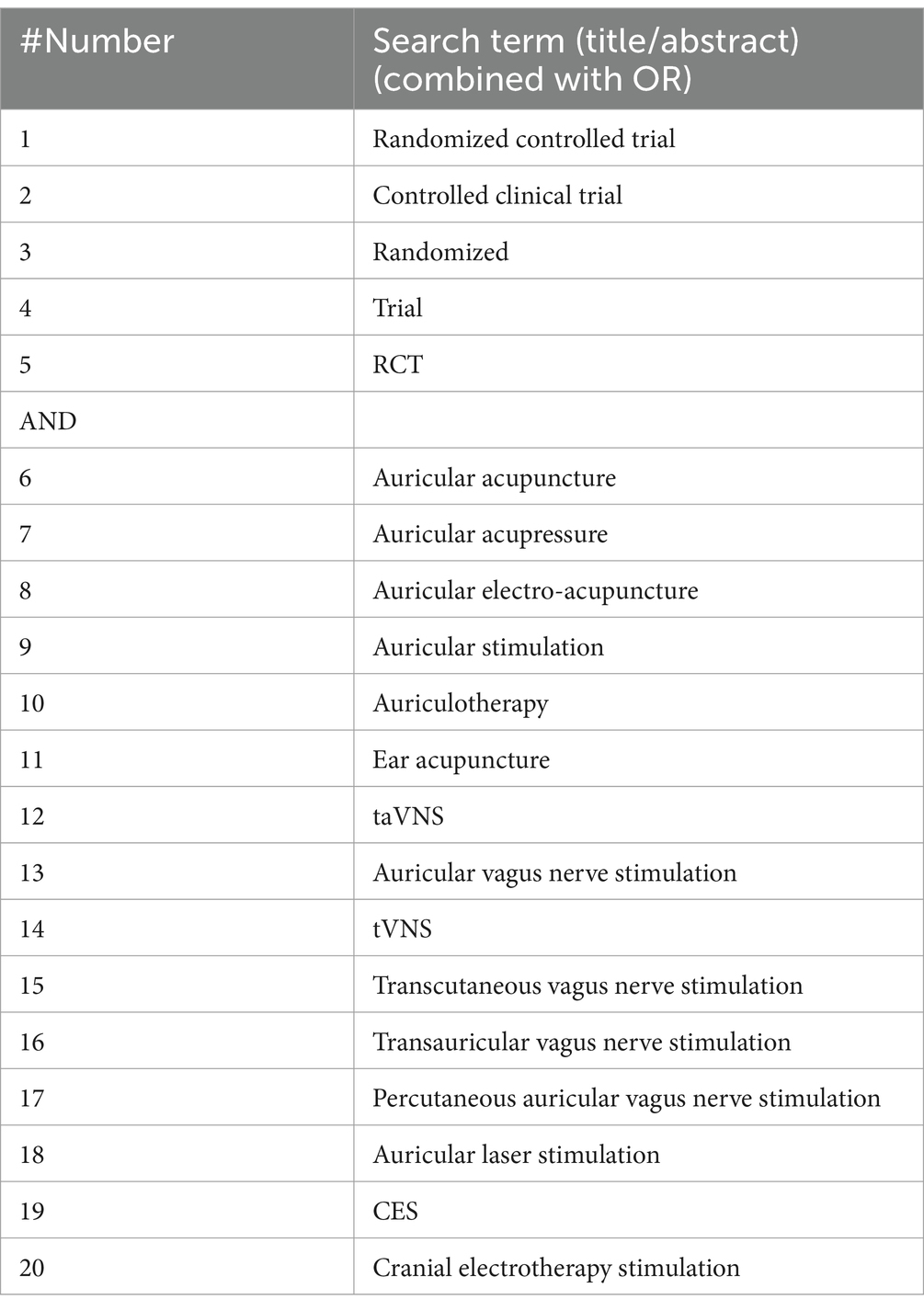
Table 1. Search strategy for the MEDLINE database.
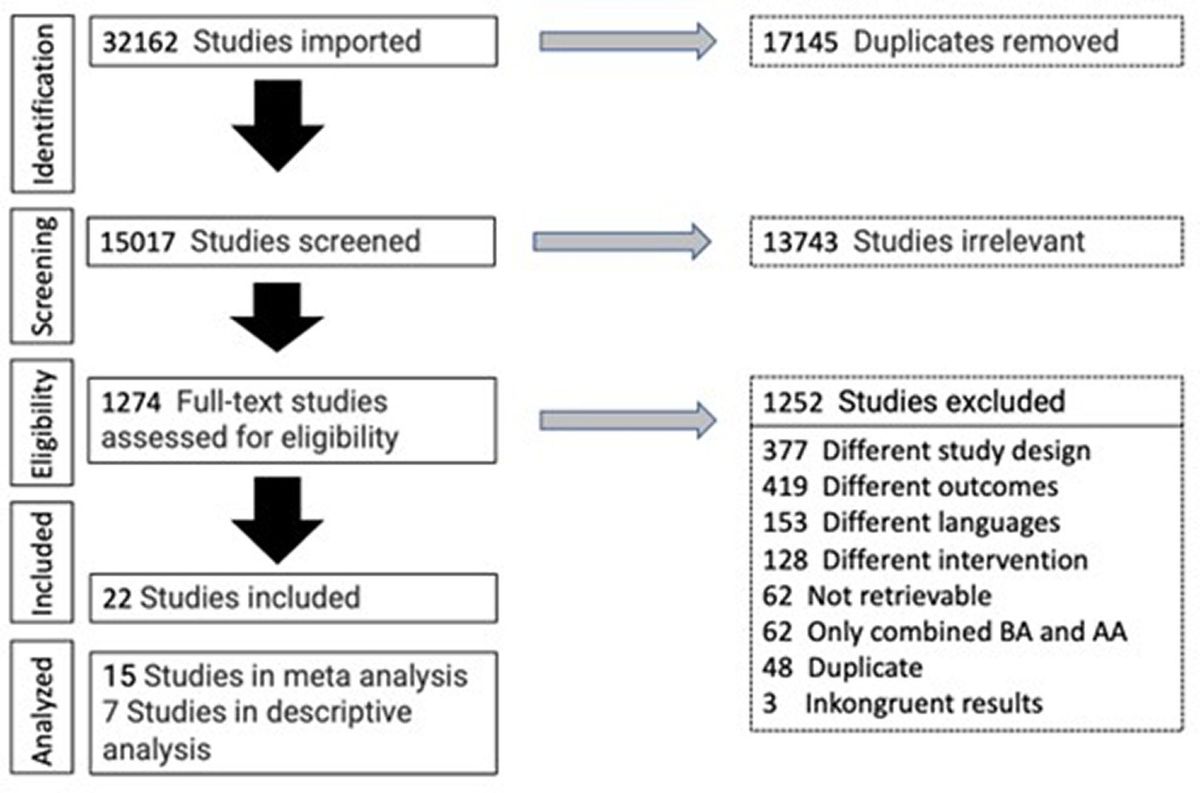
2.3 Data extraction and management 2.3.1 Trial identificationTwo researchers (JD and KH) independently reviewed: titles, abstracts, and full texts for suitability. Discrepancies were resolved by discussion with a third author (TU). If an article did not contain enough information to determine eligibility, we contacted the trial authors via email. The selection process is shown in the PRISMA flowchart in Figure 1.
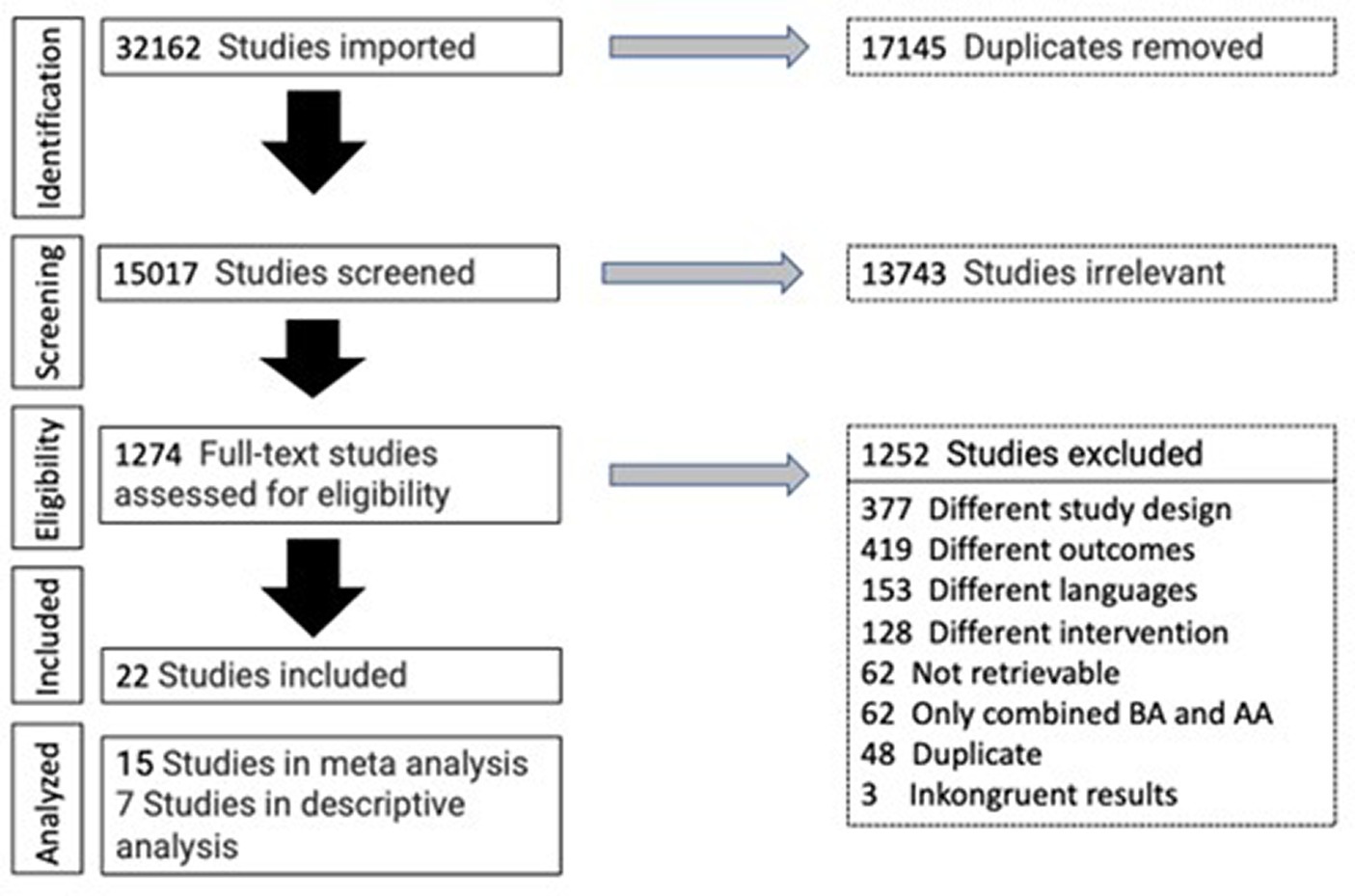
Figure 1. PRISMA flowchart.
2.3.2 Data extraction and assessment of risk of bias in included trialsJD and KH independently extracted data. The methodological quality of each RCT was assessed using the risk of bias tool I recommended in the Cochrane Handbook. A consensus process was conducted before entering the data into the Review Manager software (RevMan 5.4. 2020).
2.3.3 Measures of treatment effects and dealing with missing dataThe results of the treatment were analyzed. In cases of multiple-arm trials, only the arms that fulfilled the inclusion criteria were chosen. The outcomes presented as continuous data were analyzed as MDs with 95% confidence intervals (CIs) or standardized mean differences (SMDs). When final means were not reported, or baseline values differed in a relevant way, changes from baseline were used in the meta-analysis. According to Cochrane Handbook Chapter 10.5.2., MD was applied. If a relevant number of data were missing, this was indicated in the risk of bias section. We did not use imputation or other strategies for missing data. For non-continuous data that were not suitable for meta-analysis, the selected effect measures were analyzed descriptively.
2.3.4 Assessment of heterogeneityBecause of the broad inclusion criteria, high heterogeneity was expected. We used random-effects meta-analysis instead of fixed-effects meta-analysis when we considered high heterogeneity to be relevant. Heterogeneity was considered substantial if T2 was greater than zero and either I2 was greater than 50% or if the X2 test for heterogeneity yielded a low p-value (less than 0.10).
2.3.5 Assessment of reporting biasesA funnel plot with asymmetry was examined for each of the included trials.
2.4 Data synthesisFixed-effect meta-analyses were performed initially, in cases of high heterogeneity, random-effect analyses were performed. Data not suitable for meta-analysis were reported separately. Furthermore, for each anthropometric parameter, a GRADE assessment was undertaken.
2.4.1 Subgroup analysis and sensitivity analysisSubgroup analysis was performed to assess the effects of the different AS methods on the single obesity-related outcomes. Sensitivity analysis was considered for the outliers of the meta-analysis.
3 Results 3.1 Literature search and analysisOut of 1,274 trials that were analyzed with full-text analysis, a total of 22 met the inclusion criteria (see Figure 1).
3.2 Data extraction and analysisThe number of trial participants, gender, age, type of intervention, and assessment method for anthropometric parameters are summarized in Table 2.
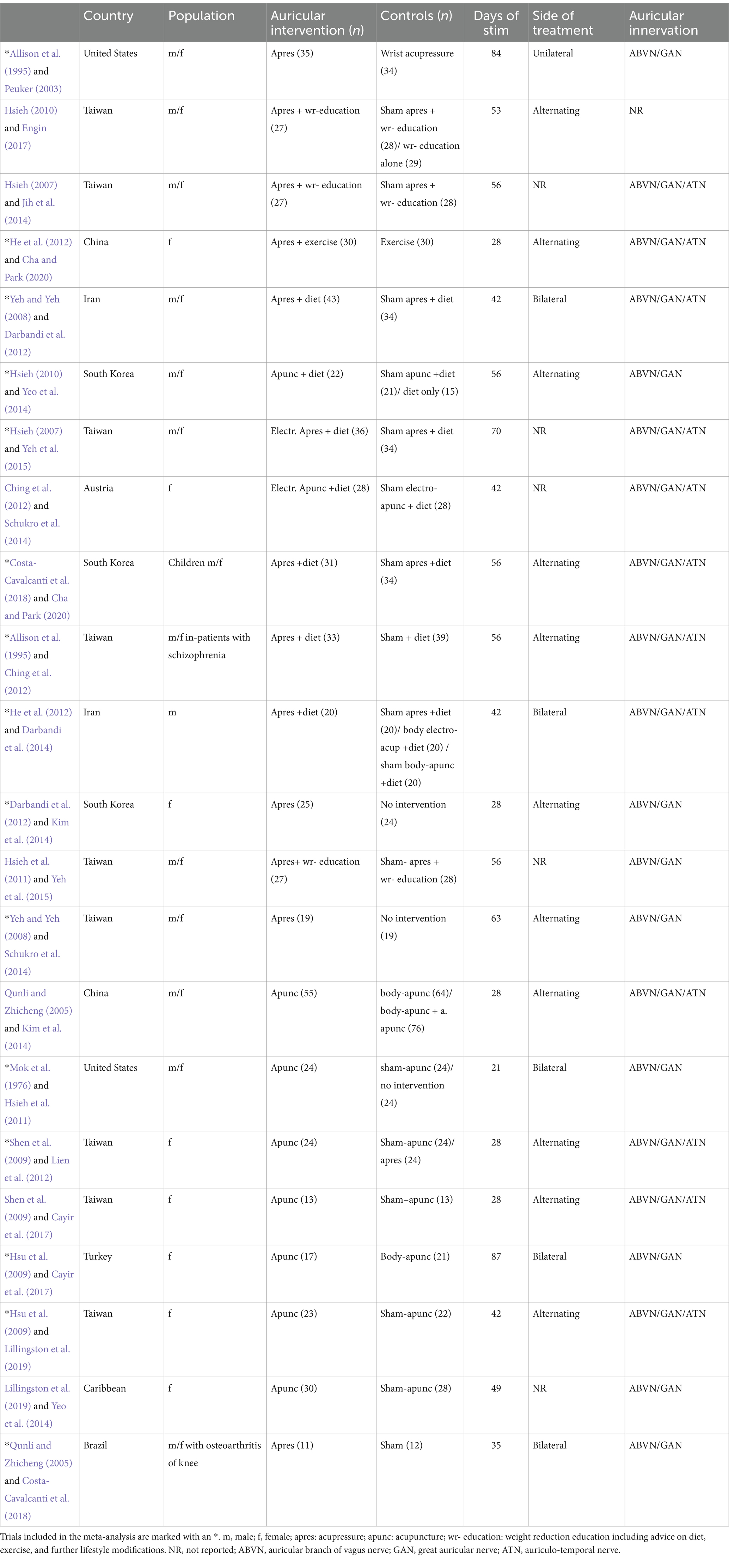
Table 2. Overview of eligible RCTs.
3.3 Baseline characteristicsA total of 1,333 individuals were included in this systematic review. A total of 91% were female subjects. One trial did not provide any information on sex concerning the included school children (Cha and Park, 2020). The age of the individuals ranged between 10 and 62 years, with a median of 35 years. One trial examined a mixed population of obese and non-obese patients (Yeh and Yeh, 2008). Obesity was defined as a BMI >25. Two studies adjusted the cutoff for obesity because of the Asian population (Hsieh, 2007, 2010). In the subgroup analysis, we pooled only the data of the obese trial participants. One trial was conducted on psychiatric in-patients (Ching et al., 2012), and another on a sample with knee osteoarthritis (Costa-Cavalcanti et al., 2018).
3.4 Comparison of trial designsSeveral study designs could be identified. Most of the studies were designed as two-armed studies (n = 16) (Allison et al., 1995; Hsieh, 2007; Yeh and Yeh, 2008; Hsu et al., 2009; Shen et al., 2009; Hsieh et al., 2011; Ching et al., 2012; Darbandi et al., 2012; He et al., 2012; Kim et al., 2014; Schukro et al., 2014; Yeh et al., 2015; Cayir et al., 2017; Costa-Cavalcanti et al., 2018; Lillingston et al., 2019; Cha and Park, 2020), followed by three-armed studies (n = 5) (Mok et al., 1976; Qunli and Zhicheng, 2005; Hsieh, 2010; Lien et al., 2012; Yeo et al., 2014) and four-armed studies (n = 1) (Darbandi et al., 2014). All the included trials were conducted on obese individuals.
3.5 InterventionThirteen RCTs used acupressure with small beads or plant seeds for stimulation (Allison et al., 1995; Hsieh, 2007, 2010; Yeh and Yeh, 2008; Hsieh et al., 2011; Ching et al., 2012; Darbandi et al., 2012, 2014; He et al., 2012; Kim et al., 2014; Yeh et al., 2015; Costa-Cavalcanti et al., 2018; Cha and Park, 2020). Auricular acupuncture with conventional needles or semipermanent needles was identified in eight studies (Mok et al., 1976; Qunli and Zhicheng, 2005; Hsu et al., 2009; Shen et al., 2009; Lien et al., 2012; Schukro et al., 2014; Yeo et al., 2014; Cayir et al., 2017; Lillingston et al., 2019). Additional electrical stimulation of the ear was used in one trial (Schukro et al., 2014). In 21 of all 22 trials, stimulation was applied in auricular regions with vagal innervation (mainly concha). One study did not provide any information about the location of AS (Hsieh, 2010).
Eleven trials used add-on AS to the use of additional weight loss interventions, such as exercise, diet, or weight reduction education, which included diet and physical exercise counseling for all treatment arms (Hsieh, 2007, 2010; Hsieh et al., 2011; Darbandi et al., 2012; Schukro et al., 2014; Yeo et al., 2014; Yeh et al., 2015). The mean duration of AS was 48 days, ranging between 21 days (Mok et al., 1976) and 87 days (Cayir et al., 2017).
3.6 ControlsDifferent control groups were identified in the included studies. The most common control group was a sham procedure (Mok et al., 1976; Hsieh, 2007, 2010; Hsu et al., 2009; Shen et al., 2009; Hsieh et al., 2011; Ching et al., 2012; Darbandi et al., 2012, 2014; Lien et al., 2012; Schukro et al., 2014; Yeo et al., 2014; Yeh et al., 2015; Costa-Cavalcanti et al., 2018; Lillingston et al., 2019; Cha and Park, 2020). Some studies have also compared AS vs. active controls (Mok et al., 1976; Hsieh, 2007, 2010; He et al., 2012; Lien et al., 2012; Wang et al., 2014; Yeo et al., 2014). These included mostly dietary instructions (Hsieh, 2007, 2010; Yeo et al., 2014) and physical exercise (He et al., 2012). Four studies also compared AS to classical body acupuncture and acupressure (Allison et al., 1995; Qunli and Zhicheng, 2005; Darbandi et al., 2014; Cayir et al., 2017). Four trials had no-intervention control (Yeh and Yeh, 2008; Kim et al., 2014).
3.7 OutcomesAll trials applied AS on regions of vagal innervation via the auricular branch of the vagus nerve (ABVN) (see Table 1 and for most frequently used points, see Figure 2). Most trials have examined the effects of AS on anthropometric parameters. Weight (n = 17) (Mok et al., 1976; Allison et al., 1995; Qunli and Zhicheng, 2005; Yeh and Yeh, 2008; Hsu et al., 2009; Shen et al., 2009; Hsieh et al., 2011; Ching et al., 2012; Darbandi et al., 2012; He et al., 2012; Lien et al., 2012; Kim et al., 2014; Schukro et al., 2014; Yeo et al., 2014; Cayir et al., 2017; Lillingston et al., 2019; Cha and Park, 2020), BMI (n = 12) (Hsieh, 2007, 2010; Yeh and Yeh, 2008; Hsu et al., 2009; Darbandi et al., 2012, 2014; He et al., 2012; Lien et al., 2012; Kim et al., 2014; Schukro et al., 2014; Yeo et al., 2014; Cayir et al., 2017; Lillingston et al., 2019), body fat (n = 6) (Allison et al., 1995; Yeh and Yeh, 2008; Darbandi et al., 2012; Kim et al., 2014; Yeo et al., 2014; Cayir et al., 2017), waist circumference (n = 6) (Yeh and Yeh, 2008; He et al., 2012; Lien et al., 2012; Darbandi et al., 2014; Yeo et al., 2014; Cayir et al., 2017), hip circumference (n = 4) (Yeh and Yeh, 2008; Lien et al., 2012; Darbandi et al., 2014; Cayir et al., 2017), and the ratio of waist and hip circumference (n = 2) (Yeh and Yeh, 2008; Kim et al., 2014). Three trials examined the effect on glucose metabolism (Hsu et al., 2009; Lien et al., 2012; Costa-Cavalcanti et al., 2018), and a total of five studies have investigated the effects related to lipid metabolism and digestive hormones (Hsu et al., 2009; Darbandi et al., 2012; Lien et al., 2012; Yeh et al., 2015; Costa-Cavalcanti et al., 2018). Of the 22 trials included in this systematic review, 15 provided sufficient data and were eligible for meta-analysis, while 7 trials were evaluated descriptively. Forest plots are only presented for pooled outcomes of five trials and more. Forest plots of four or fewer trials can be found in the Supplementary material.
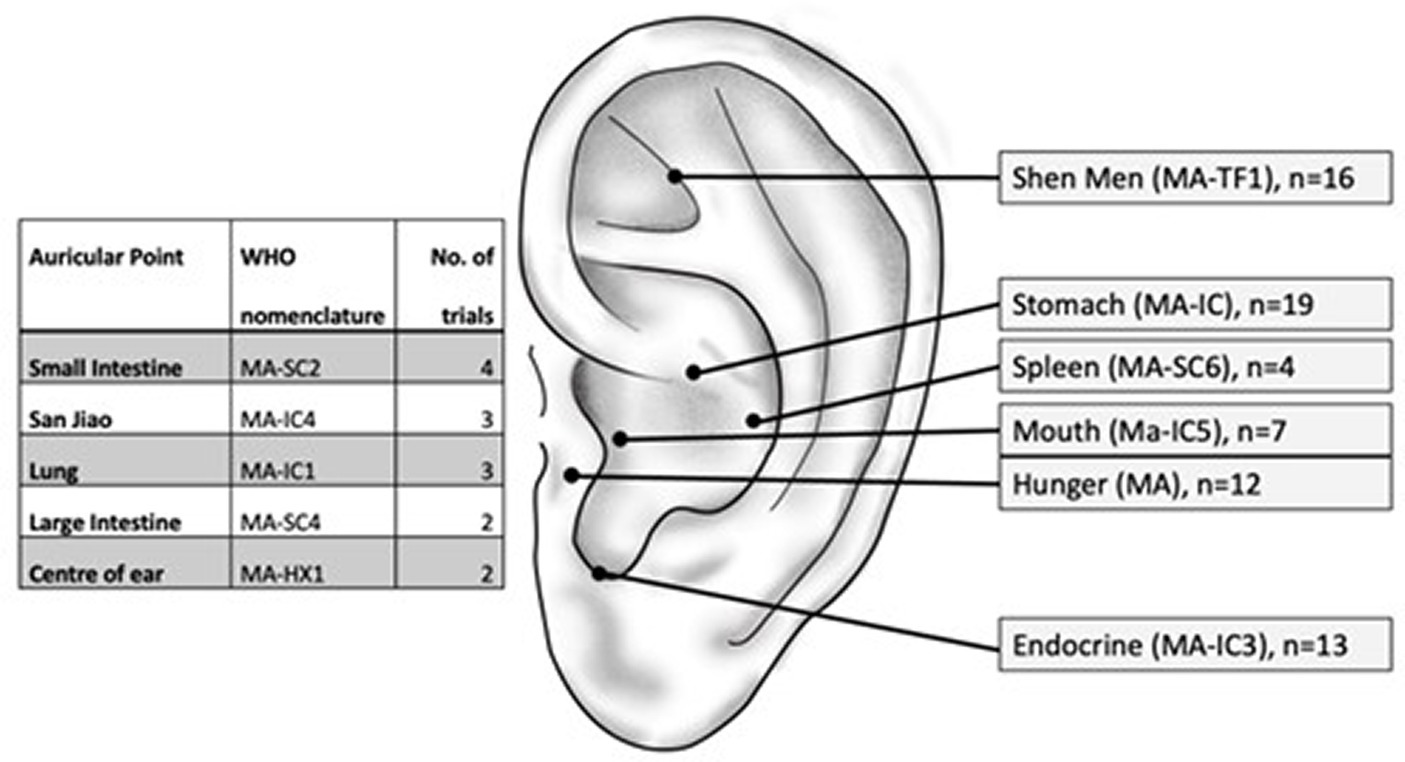
Figure 2. Auricular points used in obesity and blood lipid reduction trials. Not shown: points used in a single trial.
3.8 Body mass indexA total of 10 trials with 487 individuals provided data on BMI. Compared to the control methods, AS significantly reduced BMI (MD = −0.38 BMI points, 95% CI (−0.55 to −0.22), p < 0.0001) (see Figure 3). The strongest BMI reduction of a mean of 1.01 points was achieved in a two-armed trial by Kim et al. (2014). South Korean female obese college students were allocated to ear acupressure or waiting lists. After 1 month of continuous and self-applied ear acupressure with diet or exercise, the acupressure group lost 3.1 kg (SD 0.73) vs. 0.2 kg (SD 1.05) (difference p < 0.001) and 1.23 (SD 0.34) BMI points vs. 0.15 (SD 0.45) BMI points (difference p < 0.001) compared to the control group in the pre-post calculation. The authors explained that satisfying results were connected to self-treatment and an increased feeling of self-efficacy. A similar reduction of weight and BMI was achieved in the sham-controlled trial of Lien et al. Taiwanese obese women received auricular true or sham acupuncture. Regular diets were maintained throughout the study. After 1 month of ear acupuncture with semipermanent needles, the real acupuncture group had a mean of 1.3 kg (SD 2.2) vs. 0.6 kg (SD 1.4) and a BMI of 0.5 points (SD 0.9) vs. 0.2 points (SD 0.5) in the sham acupuncture group.
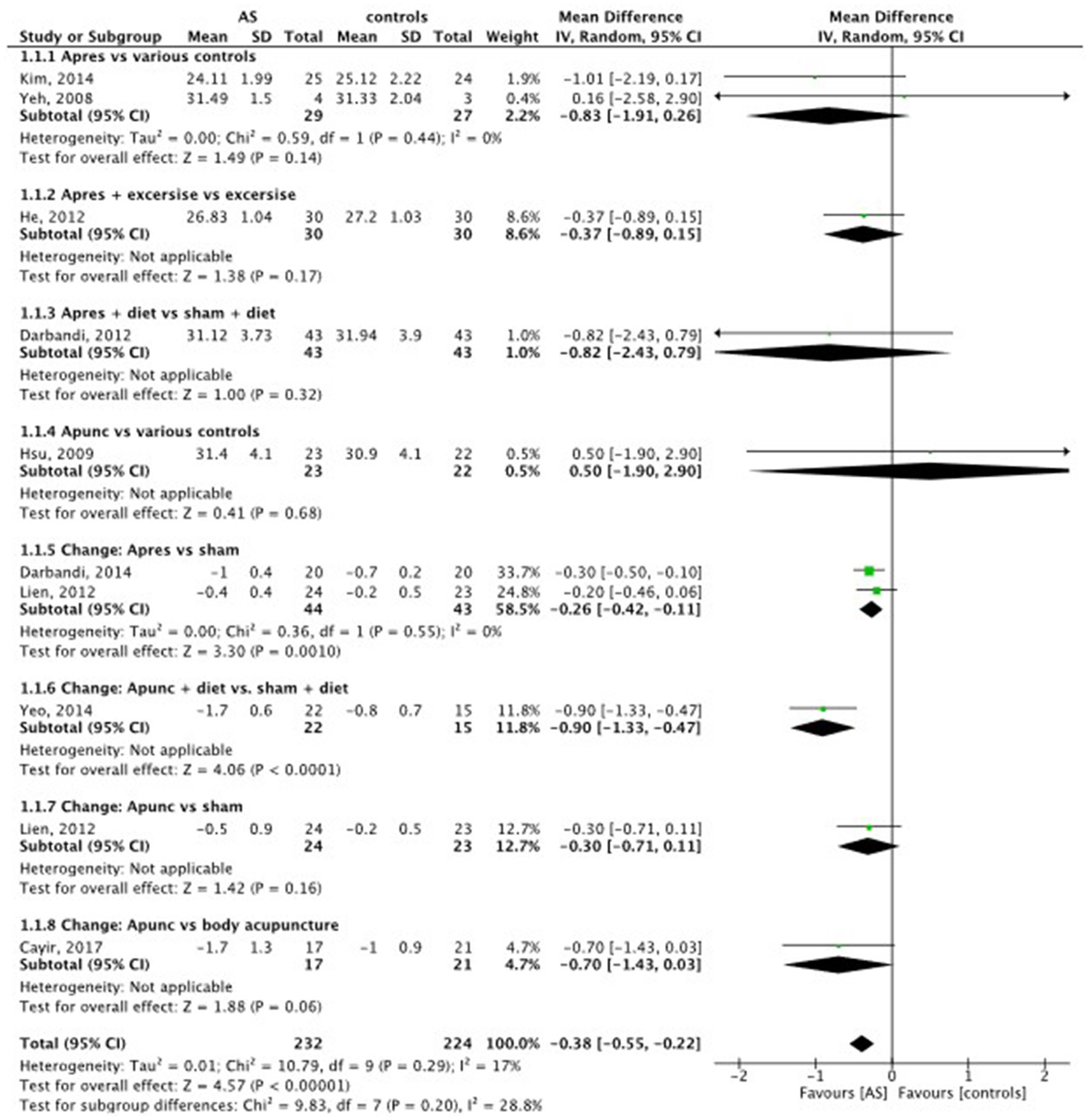
Figure 3. Body mass index (BMI): AS vs. controls.
3.9 WeightIn 12 trials with data on the body weight of 655 individuals, compared to the control methods, AS led to a significant reduction of body weight (MD = −0.66 kg, 95% CI (−1.12 to −0.20), p = 0.005) (see Figure 4).
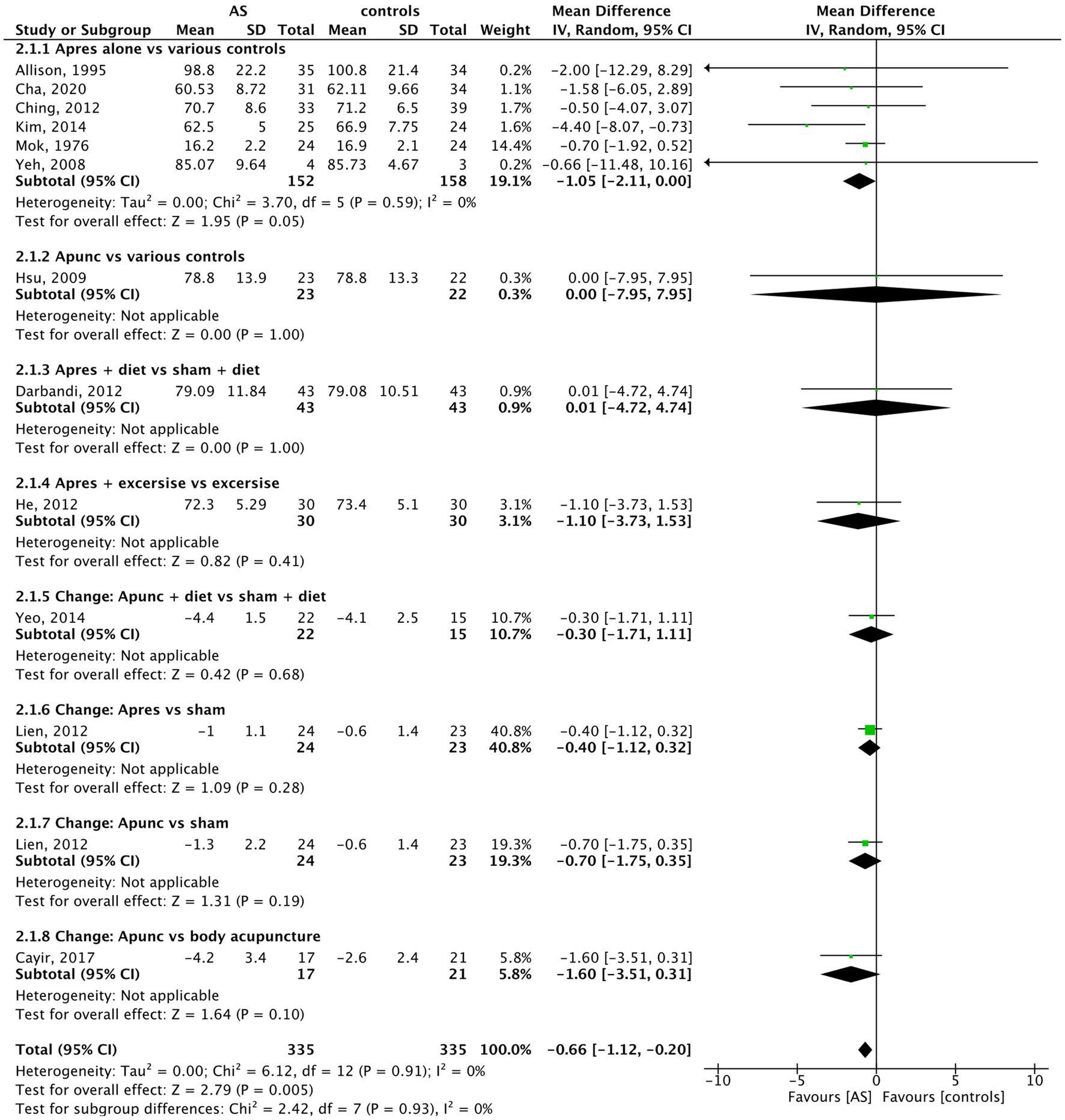
Figure 4. Weight: AS vs. controls.
No significant difference, despite a low-calorie diet, could be achieved with add-on acupressure compared to add-on sham acupressure in Iranian obese men after 6 weeks of treatment (Darbandi et al., 2014).
3.10 Body fatData of 6 trials with 317 individuals were included in the analysis of body fat. In body fat percentage, compared to the control methods, AS did not show a significant effect on reducing the amount of body fat (MD = −1.21, 95% CI (−2.47 to 0.05), p = 0.06) (see Figure 5). Body fat was mostly measured with the method of impedance analysis. Cayir et al yielded the highest body fat percentage reduction from a baseline of 5.6% (SD5.3) with auricular acupuncture vs. 2.0% (SD2.8) with body acupuncture. No additional measures were used by the patients, and both acupuncture forms were applied two times per week over 12 weeks.
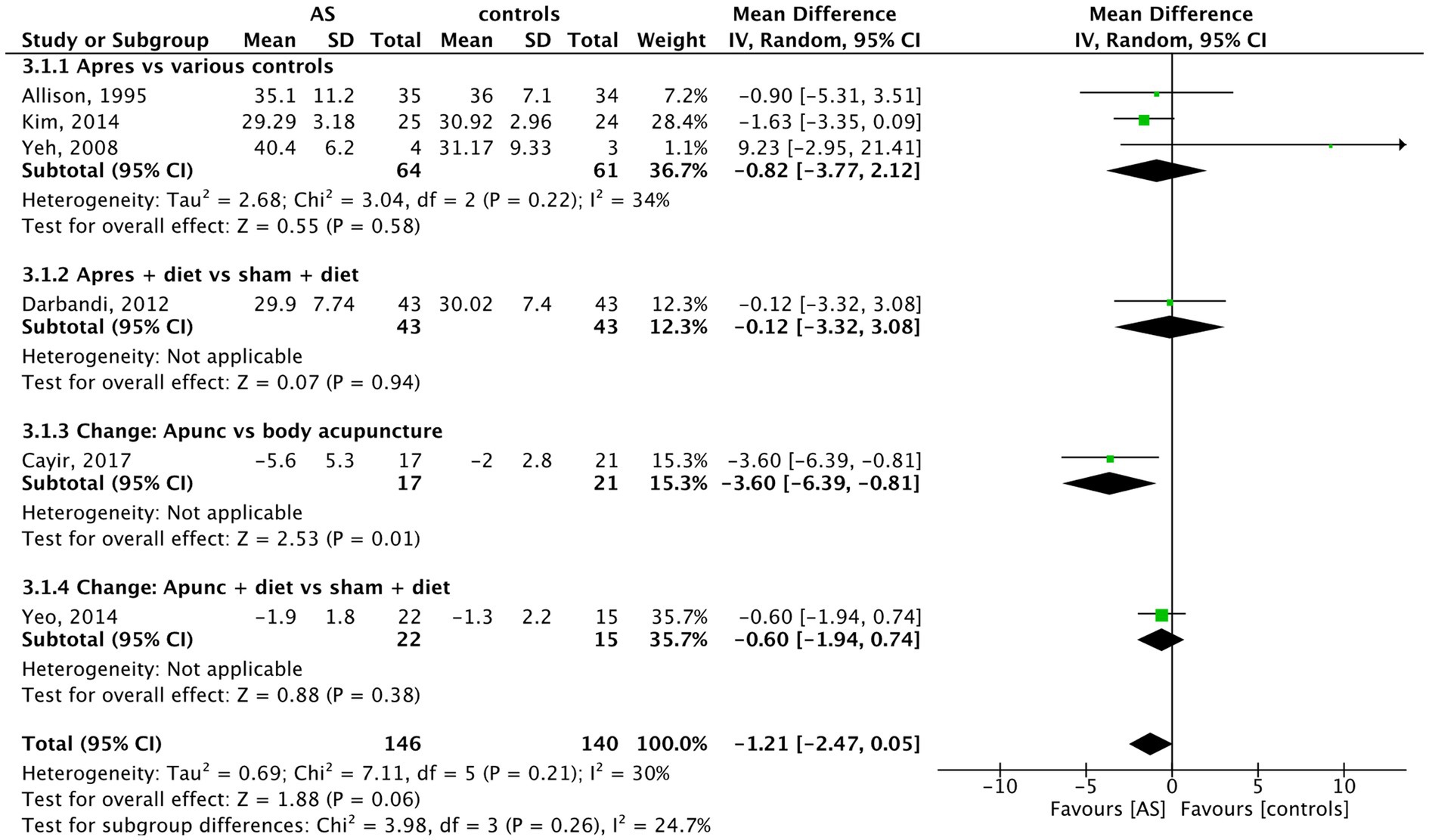
Figure 5. Body fat: AS vs. controls.
3.11 Waist circumferenceIn the analysis of the six trials with data on waist circumference of 276 individuals, compared to the control methods, AS reduced waist circumference significantly (MD = −1.44 cm, 95% CI (−2.69 to −0.20), p = 0.02) (see Figure 6). The biggest decrease was achieved in the trial by Darbandi et al. (2014), who randomized 80 obese participants in four groups: body electroacupuncture (A), auricular acupressure (C), sham body electroacupuncture (B), and sham auricular acupressure (D). From the auricular acupressure vs. sham auricular acupressure arms (n = 2×20), it was possible to use the data for meta-analysis. All subjects received a 500 kcal low-calorie diet. Only the verum auricular acupressure led to a relevant reduction of hip and waist circumference after 6 weeks of treatment compared to sham (Darbandi et al., 2014).
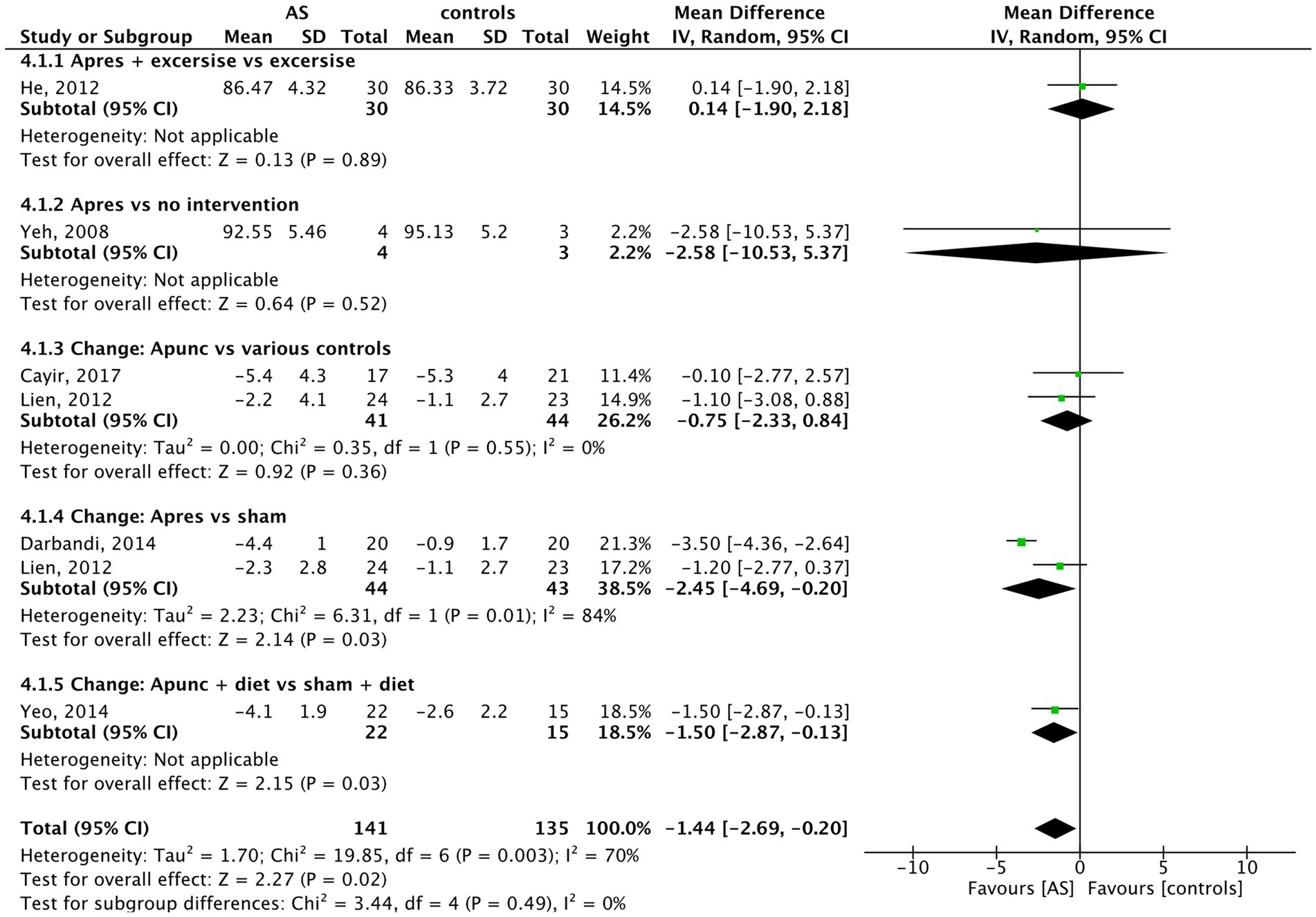
Figure 6. Waist circumference: AS vs. controls.
Regarding the pooled data from four or fewer trials (see forest plots in the Supplementary material), a positive effect on obesity-related metabolic parameters was observed only in the comparisons of leptin, insulin, and HOMA insulin resistance. Compared to the control methods, AS had a significant effect on reducing leptin (4 trials, n = 295, SMD = −0.40, 95% CI (−0.63 to −0.17), p = 0.0008). Regarding insulin, AS had a significant effect on reducing fasting insulin serum level (3 trials, n = 139, MD = −3.50 UI/ml, 95% CI (−6.59 to −0.41), p = 0.03) and HOMA insulin resistance (3 trials, n = 139, MD = −1.06, 95% CI (−2.03 to −0.09), p = 0.03).
No significant effects of AS compared to control methods were found in the meta-analyses of hip circumference, ratio of waist/hip circumference, cholesterol, LDL, triglycerides, adiponectin, and ghrelin (see Supplementary material). Only one trial examined the impact of glucose levels in obese patients (Costa-Cavalcanti et al., 2018). No significant difference was reported between the groups.
3.12 Sensitivity analysisFor details, see Tables 3, 4. We performed two sensitivity analyses: First, positive outliers were excluded from the meta-analysis.
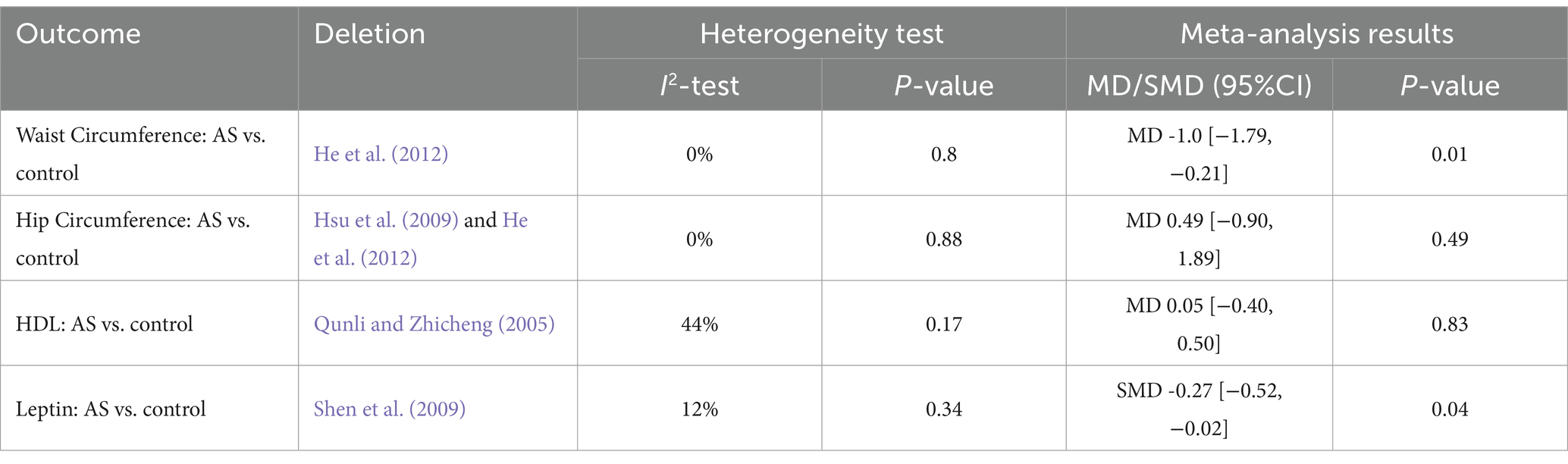
Table 3. Sensitivity analysis: heterogeneity.
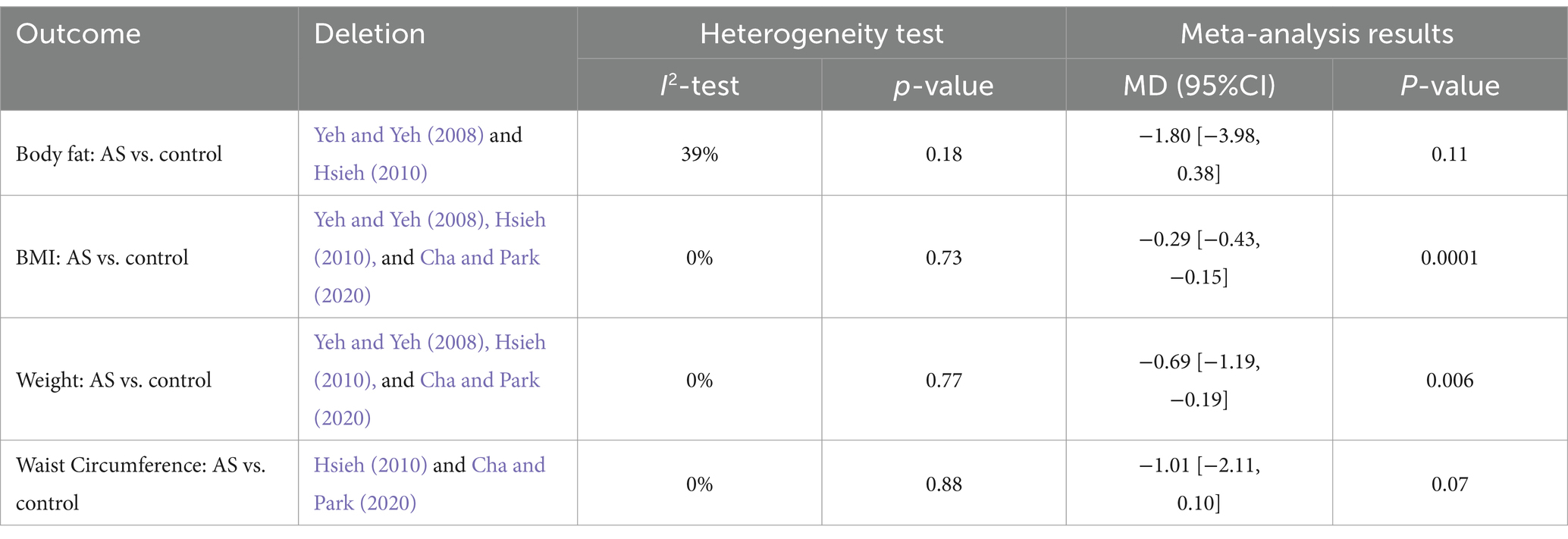
Table 4. Sensitivity analysis: additional therapy.
Second, trials with additional interventions besides AS were excluded. In the case of waist circumference and leptin, significant results could be still obtained, excluding positive outliers.
Regarding the sensitivity analysis of AS, excluding additional interventions such as dietary advice or physical exercise, we still found a significant benefit of AS alone for reducing BMI and weight.
3.13 Descriptive analysis of studiesThere were seven trials that did not have continuous data for quantitative meta-analysis. In Table 5, the dichotomous outcomes are summarized.
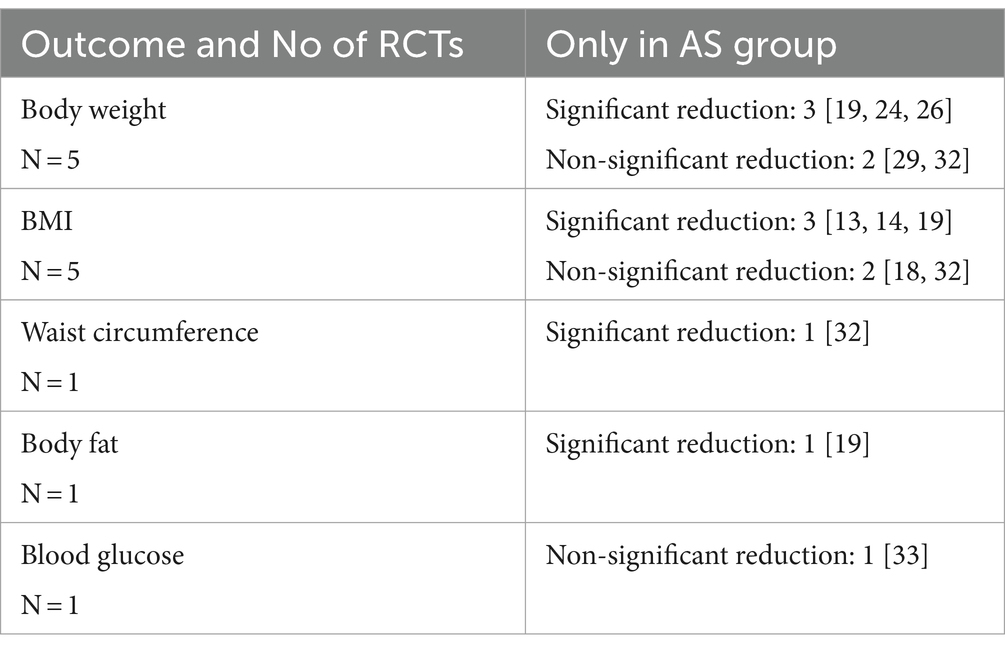
Table 5. Results of descriptive analysis.
3.14 Safety of interventionOf the 22 included studies, adverse events were recorded in 12 studies. Six study groups could not document any adverse side effects (Mok et al., 1976; Yeh and Yeh, 2008; Darbandi et al., 2012, 2014; Cayir et al., 2017; Cha and Park, 2020). Minor side effects were recorded in five trials (Allison et al., 1995; Hsu et al., 2009; Ching et al., 2012; Lien et al., 2012; Schukro et al., 2014). One study described in its methodology that they recorded adverse side effects. However, no information could be extracted from the results (Yeh et al., 2015).
Common side effects of AS that have been reported are all mild and include pain or minor bleeding at the stimulation side (four trials), transient dizziness (three trials), erythema (two trials), and skin irritation (two trials).
3.15 Quality assessmentThe overall study quality was moderate (see Figures 7, 8). A funnel plot was performed and revealed no publication bias.
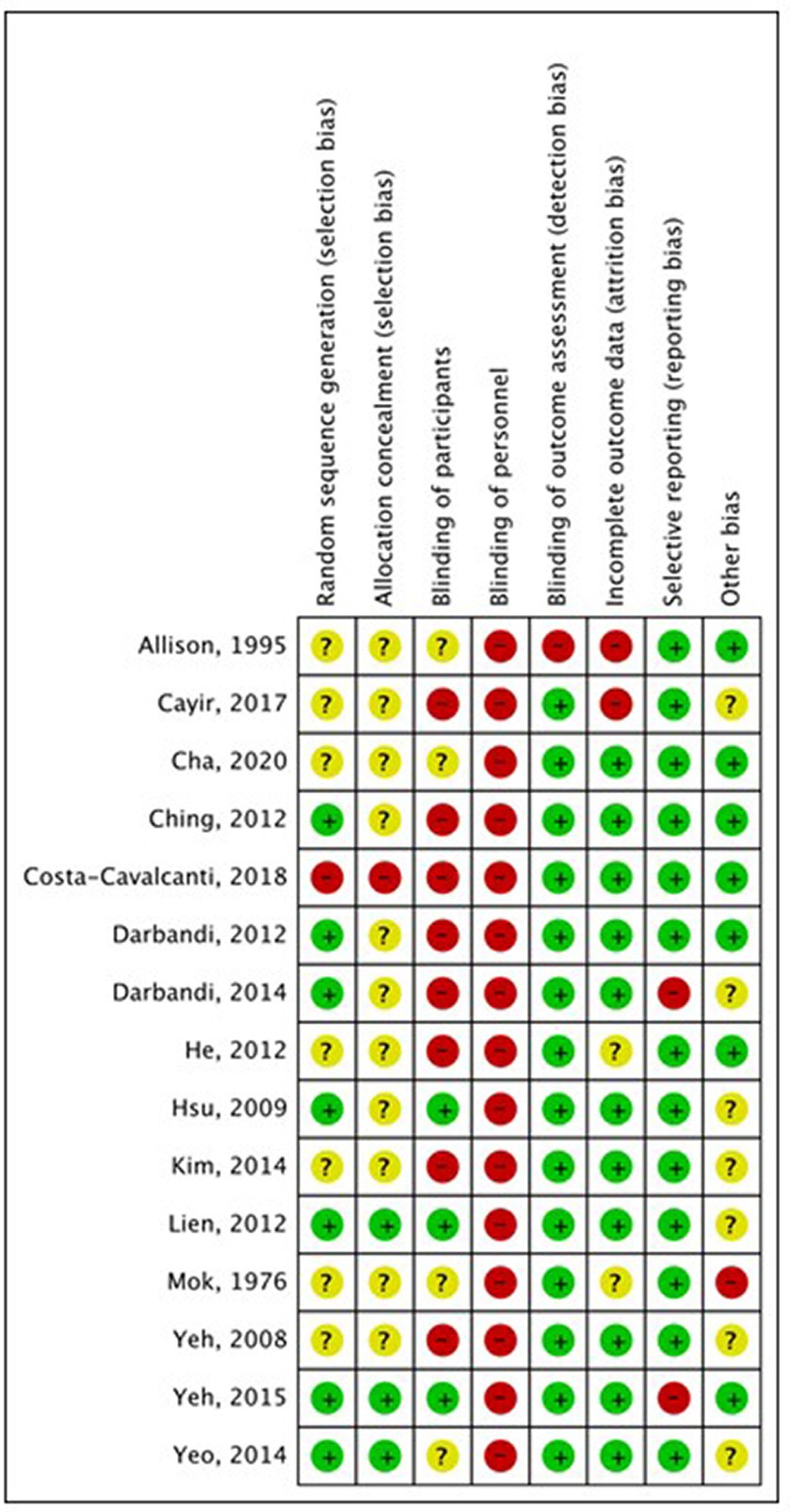
Figure 7. Risk of bias assessment. +: low risk of bias; –: high risk of bias;?: unclear risk of bias.
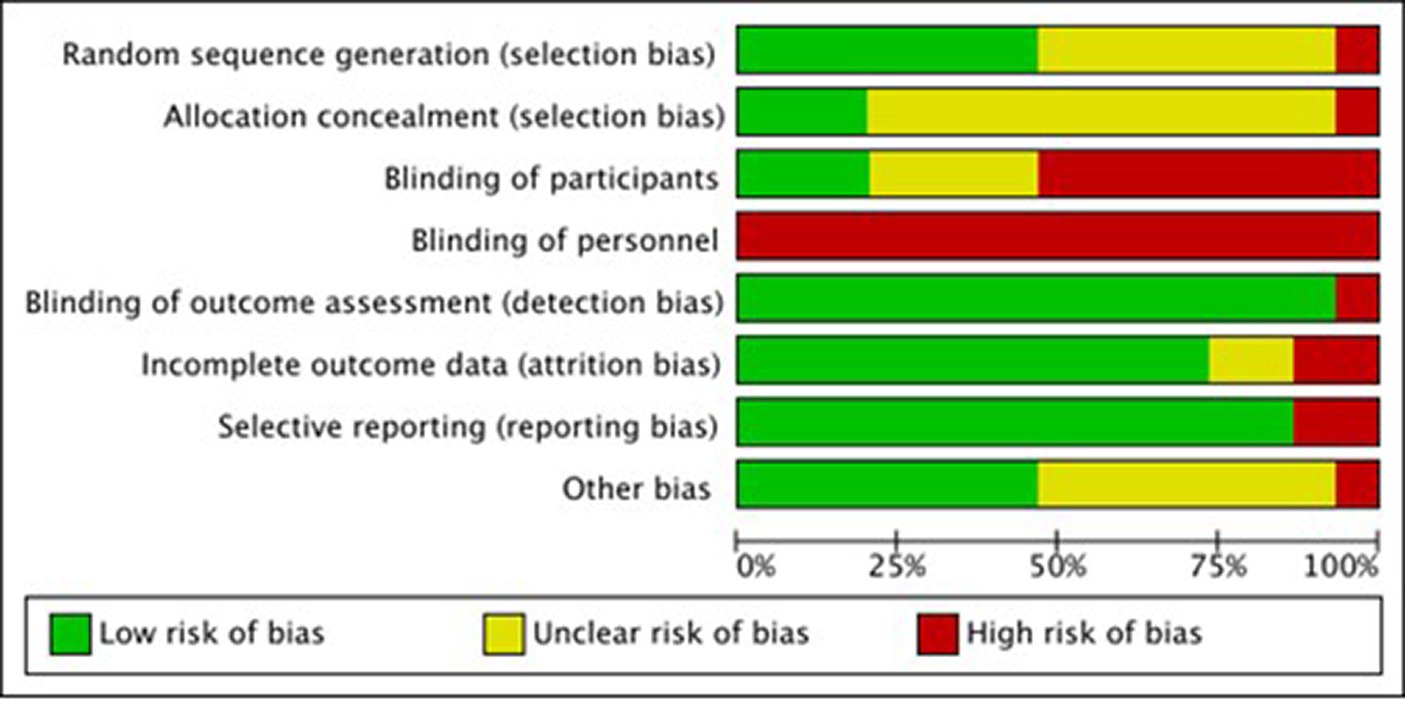
Figure 8. Risk of bias summary.
3.16 Excluded studiesOne trial had several contradictions in the tables, and we judged it prudent to exclude it from the evaluation (Abdi et al., 2012).
3.17 Funding sourcesMost study groups had not provided funding information (Mok et al., 1976; Qunli and Zhicheng, 2005; Hsieh, 2007, 2010; Shen et al., 2009; Hsieh et al., 2011; Lien et al., 2012; Kim et al., 2014; Schukro et al., 2014). For the most part, the studies were supported either by the research group itself (Hsu et al., 2009; Darbandi et al., 2012, 2014; Yeh et al., 2015; Cayir et al., 2017; Lillingston et al., 2019) or by the government (Yeh and Yeh, 2008; Ching et al., 2012; Yeo et al., 2014; Costa-Cavalcanti et al., 2018; Cha and Park, 2020). Individual studies were funded by a company (Allison et al., 1995) or an acupuncture society (He et al., 2012).
4 DiscussionThe results of the meta-analysis demonstrated that a reduction in weight and BMI compared to controls was achieved by AS of the auricular regions that receive afferent vagal nerve supply in obese patients. The achieved mean reductions measured—despite additional diets, exercise programs, and a mean of 50 days of treatment—were marginal, and did not reach the 5% reduction of body weight that is considered clinically meaningful (Williamson et al., 2015).
The weight reduction achieved in this meta-analysis is in the range of physiological weight fluctuations over the day (Simkin-Silverman et al., 1998; Field et al., 2001); on the other hand, some trials offered exercise programs for both the intervention and control groups, so an increase in muscle mass might have concealed the loss of body fat in the weight measurements. Regarding obesity-related hormones, the clinical significance of the results remains elusive due to the small sample size.
Interestingly, acupressure had comparable or bigger effects than acupuncture, possibly due to the continuous stimulation, as the pellets remained plastered in situ for weeks and patients were instructed to press them daily. This effect has been observed in past research on AS (Usichenko et al., 2022). This effect, though, could have had an impact on sham needles with a missing needle tip. The plasters contain a metal ring, which might have had a stimulating effect, too, when massaged.
In the analysis of the safety aspects of the different forms of AS, only minor side effects have been reported in the included studies, which is in line with the results of a review of reviews of the risks and safety of extended auricular therapy (Nielsen et al., 2020). Throughout the trials, a moderate quality was found. The analysis of study quality was performed with the RoB tool 1 from the Cochrane handbook, which was chosen for reasons of stricter judgment.
Interestingly, a relevant weight reduction was not achieved by diets either; this fact has been described before in other systematic reviews comparing different diets (Naude et al., 2022).
Exercise seems more promising–a recently published systematic review with meta-analysis investigated the influence of dancing compared to no intervention on the parameters of obesity in 10 RCTs with 650 overweight and obese participants. The dancing corresponded to the weekly amount of exercise recommended by the World Health Organization (WHO) (150–300 min). The duration of the intervention was 42–84 days. They were able to achieve an average BMI reduction of 1.03 kg/m2 (95% CI -1.63 to −0.44; p = 0.0006) (Zhang et al., 2024).
The effects of vagal stimulation at the auricle on stress response and cardiovascular parameters have been proven in numerous previous studies (Qu et al., 2014; Usichenko et al., 2022; Hua et al., 2023; Sigrist et al., 2023). It remains to be determined, if the mechanism behind the weight loss via AS is linked to an altered stress response, in the face of calorie reduction.
The strength of this review is that it included more RCTs and more anthropometric and blood chemistry values than previous reviews and it presents an overview of the most frequently stimulated points. The present findings are comparable to a systematic review and meta-analysis published in 2020, in which the effects of AS were analyzed in a smaller sample of trials with limited outcomes (Mendonça et al., 2020). In the meta-analysis of five trials, BMI was reduced by a mean of 0.86 kg/m2 (95% CI, 0.533–1.196; p < 0.004) and weight by 1.5 kg (95% CI, 0.606–2.407; p < 0.0001). In this review by Mendoca et al., the mean achieved body weight reduction still does not reach a clinically significant 5% of body weight, nor does it reach a full point of BMI in the calculated total difference (Mendonça et al., 2020). Limitations: A limiting factor to the present systematic review is that only studies in English were finally included in this analysis. Auriculotherapy has long been used in traditional medical systems such as Chinese medicine; however, scientific contributions in Chinese, Korean, and Japanese are missing in this review, and their influence on the evidence remains unclear. Although we tried to compare the outcomes that were assessed at the end of the treatment, there is substantial heterogeneity in the duration of intervention, which might be a further limitation. Regarding the heterogeneity of control groups, we tried to account for it with clustering in subgroups. Another limitation of the results of this review is the inclusion of sham controls that might not be inert. Though the trial might give an indicator of the specific effects of certain regions of the auricle, every stimulation of the auricle, no matter the region, leads to sensory afferences leading to some kind of body reaction. This issue has been discussed extensively in the literature regarding sham points in body acupuncture (Lee et al., 2023, 2024).
Future ear acupuncture trials should take into account that there are no “inert” regions on the auricle, and even an “empty” plaster as sham control might exert an effect when massaged. Therefore, while the effect does not appear to be clinically relevant, the size of the effect may be underestimated due to active sham trials. Another bias is the high possibility of unblinding as a result of the long duration of stimulation (Usichenko and Cummings, 2024), such as plasters falling off to reveal the status of sham or real needles.
5 ConclusionThis study suggests an effect of AS in the treatment of obesity, but the size of the effect does not appear to be of clinical relevance, though it may be underestimated due to active sham trials. Regarding the influence of AS on metabolic parameters such as blood lipids and obesity-related hormones, more research is needed.
Data availability statementThe original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author/s.
Author contributionsKH: Data curation, Formal analysis, Investigation, Writing – original draft. TU: Conceptualization, Supervision, Validation, Writing – review & editing. MC: Conceptualization, Methodology, Validation, Writing – review & editing. MB: Writing – review & editing. SW: Methodology, Supervision, Validation, Writing – review & editing. BB: Funding acquisition, Supervision, Validation, Writing – review & editing. JD: Conceptualization, Formal analysis, Investigation, Project administration, Resources, Supervision, Writing – original draft.
FundingThe author(s) declare that financial support was received for the research, authorship, and/or publication of this article. KH received a research grant from the International Society of Chinese Medicine, Societas Medicinae Sinensis, Munich, Germany. The society had no role in the development of the protocol.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnins.2024.1393826/full#supplementary-material
AbbreviationsRCT, randomized controlled trial; AA, auricular acupuncture; AS, auricular stimulation; CES, cranial electrotherapy stimulation; CI, confidence intervals; SMD, standardized mean differences; RE, random effects; RoB, risk of bias; taVNS, transauricular vagus nerve stimulation; tVNS, transcutaneous vagus nerve stimulation; n/a, not available; aur. Pres., auricular acupressure; aur. Punc., auricular acupuncture; elec. Stim., electro stimulation; no inter., no intervention; sham pres., sham acupressure; sham punc, sham acupuncture; sham elec., sham electro stimulation; body punc., body acupuncture.
ReferencesAbdi, H., Abbasi-Parizad, P., Zhao, B., Ghayour-Mobarhan, M., Tavallaie, S., Rahsepar, A. A., et al. (2012). Effects of auricular acupuncture on anthropometric, lipid profile, inflammatory, and immunologic markers: a randomized controlled trial study. J. Altern. Complement. Med. 18, 668–677. doi: 10.1089/acm.2011.0244
PubMed Abstract | Crossref Full Text | Google Scholar
Allison, D., Kreibich, K., Heshka, S., and Heymsfield, S. B. (1995). A randomised placebo-controlled clinical trial of an acupressure device for weight loss. Int. J. Obes. Relat. Metab. Disord. 19, 653–658
PubMed Abstract | Google Scholar
Cayir, Y., Set, T., and Kosan, Z. (2017). The effects of auricular and body acupuncture in turkish obese female patients: a randomized controlled trial indicated both methods lost body weight but auricular acupuncture was better than body acupuncture. Acupunct Electrother. Res. 42, 1–10. doi: 10.3727/036012917X14908026364990
PubMed Abstract | Crossref Full Text | Google Scholar
Ching, H.-Y., Wu, S. L., Chen, W. C., and Hsieh, C. L. (2012). Effects of auricular acupressure on body weight parameters in patients with chronic schizophrenia. Evid. Based Complement. Alternat. Med. 2012, 1–8. doi: 10.1155/2012/151737
PubMed Abstract | Crossref Full Text | Google Scholar
Costa-Cavalcanti, R. G., de Sá-Caputo, D. C., Moreira-Marconi, E., Küter, C. R., Brandão-Sobrinho-Neto, S., Paineiras-Domingos, L. L., et al. (2018). Effect of auriculotherapy on the plasma concentration of biomarkers in individuals with knee osteoarthritis. J. Acupunct. Meridian Stud. 11, 145–152. doi: 10.1016/j.jams.2018.05.005
PubMed Abstract | Crossref Full Text | Google Scholar
Darbandi, M., Darbandi, S., Mobarhan, M. G., Owji, A. A., Zhao, B., Iraji, K., et al. (2012). Effects of auricular acupressure combined with low-calorie diet on the leptin hormone in obese and overweight Iranian individuals. Acupunct. Med. 30, 208–213. doi: 10.1136/acupmed-2011-010121
PubMed Abstract | Crossref Full Text | Google Scholar
Darbandi, M., Darbandi, S., Owji, A. A., Mokarram, P., Mobarhan, M. G., Fardaei, M., et al. (2014). Auricular or body acupuncture: which one is more effective in reducing abdominal fat mass in Iranian men with obesity: a randomized clinical trial. J. Diabetes Metab. Disord. 13, 1–7. doi: 10.1186/s40200-014-0092-3
Crossref Full Text | Google Scholar
Engin, A. (2017). The definition and prevalence of obesity and metabolic syndrome. Obes. Lipotoxicity 1, 1–17. doi: 10.1007/978-3-319-48382-5_1
Crossref Full Text | Google Scholar
Field, A., Wing, R. R., Manson, J. E., Spiegelman, D. L., and Willett, W. C. (2001). Relationship of a l
留言 (0)