CFT is a relatively rare benign fibrous lesion that typically occurs in the soft tissues of the extremities, trunk, and neck, and rarely in the pleura. According to the bibliographic research of 157 cases by Chorti et al. in 2016 [4], the stomach (18%), small intestine (8.7%), and pleura (9.9%) are the most frequent sites of occurrence of CFT. The pathologic features of CFT are the proliferation of collagenous fibrous tissue with inflammatory cell infiltration and the presence of psammoma bodies. The etiology of CFT is not clear. However, CFT has been suggested to be an inflammatory pseudotumor caused by reactive changes involving osteopontin, a cytokine expressed during the repair process of inflammation. Osteopontin induces fibroblasts to form collagenous tissue and may also be involved in the formation of sand grain-like calcification [5]. As recently as 2002, the World Health Organization established the name “calcifying fibrous tumor” in its classification of soft tissue and bone tumors [6].
We conducted a literature search (January 1999 through December 2023) in the PubMed database and the Ichushi-Web database of the Japanese Medical Abstract Society (http://login.jamas.or.jp/; NPO Japan Medical Abstracts Society) using the keywords “calcifying fibrous tumor” and “pleura”. The 41 reported cases of CFT of pleural origin to date, including the present case, are summarized in Table 1 [3, 5,6,7]. The mean age of the 41 patients was 35 years (range, 15 weeks–59 years). None of the patients was aged > 65 years. CFT is more common in young females, with a male-to-female ratio of 14:27. Twenty-five patients had multiple lesions while 16 patients had single lesions. Eighteen patients had non-specific symptoms and 23 patients were asymptomatic. All 42 patients were divided into two groups: complete resection group (n = 28) and incomplete resection group (13 cases including one who did not undergo surgery), and their characteristics were compared and analyzed (Table 2). There were no significant differences in age (p = 0.576), gender (p = 0.386), or symptoms (p = 0.6324) between the two groups. Complete resection was possible in all 15 patients with solitary tumors, but the complete resection rate for multiple tumors was significantly lower (50%) compared to the solitary tumors. Multiple lesions extending the bilateral thoracic cavity or extensively throughout the entire region, both vertical or horizontal, were more likely to be unresectable, although not statistically significant. Reasons for incomplete resection on intraoperative findings included disseminated lesions in three cases, multifocal tumors in different sites in five cases, misdiagnosis in one case and not described in three cases; in one case, tumor resection was not chosen due to the presence of similar tumors in the thoracic and abdominal cavity on CT scan. There were no reports of tumor invasion making resection impossible. In the complete resection group, thoracoscopic surgery was twice as common as open thoracotomy, and the same ratio for the incomplete resection group. The median follow-up was shorter than 2 years in both groups, and no recurrence was reported in cases of complete resection group. On the other hand, in the incomplete resection group, one case of recurrence (details unknown) [7] and five cases of residual tumor were reported to have shown no growth.
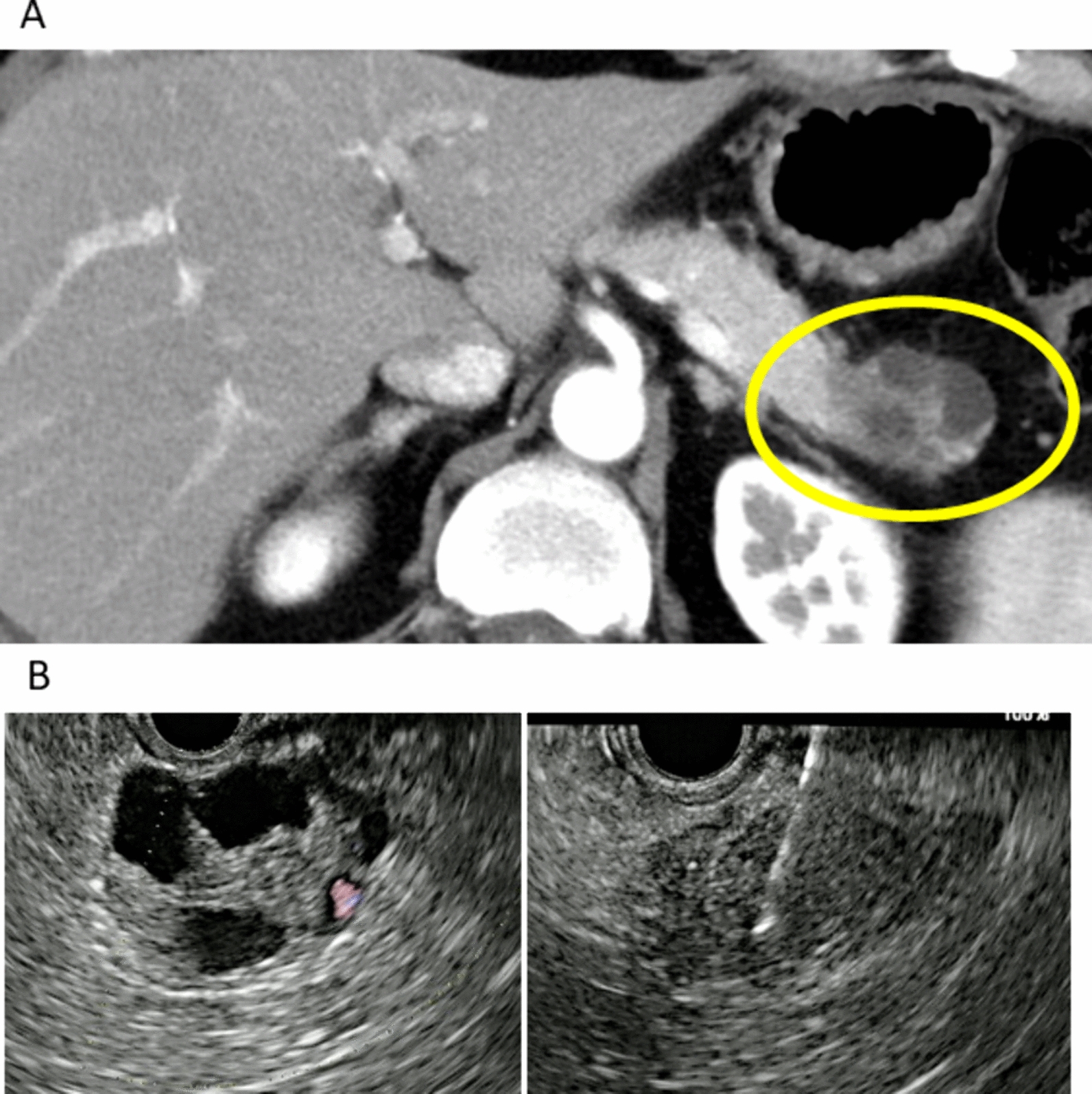
Table 1 Reported cases of pleural calcifying fibrous pseudotumorTable 2 Characteristics of patients with complete or incomplete resection of pleural calcifying fibrous pseudotumorThe differential diagnosis of pleural CFTs includes inflammatory myofibroblastic tumors, solitary fibrous tumors [8], sarcomatoid and desmoplastic mesothelioma, desmoid fibromatosis, leiomyoma, chronic fibrous pleuritis, and IgG4-related sclerosing disease. Immunostaining is useful in the differential diagnosis of these diseases. However, the lack of specific findings in CFT makes preoperative diagnosis difficult, even with CT-guided or endoscopic ultrasound needle biopsy. Furthermore, because of the difficulty in differentiating these diseases by imaging, complete resection for definitive diagnosis should be performed in cases with tumor enlargement and subjective symptoms. Mehrad et al. [7] recently reported deleterious mutations in three genes, Zinc Finger Protein 717 gene (ZNF717), Facioscapulohumeral muscular dystrophy-1 gene (FRG1), and cell division cycle 27 (CDC27), and abnormal copy number loss in chromosomes 8 and 6 by whole genome sequencing in CFT patients, suggesting that these molecular-level changes may contribute to the genesis of CFTs. Although the molecular profile of previously reported CFT cases has been examined to identify possible driver mutations, this patient did not consent to genetic testing.
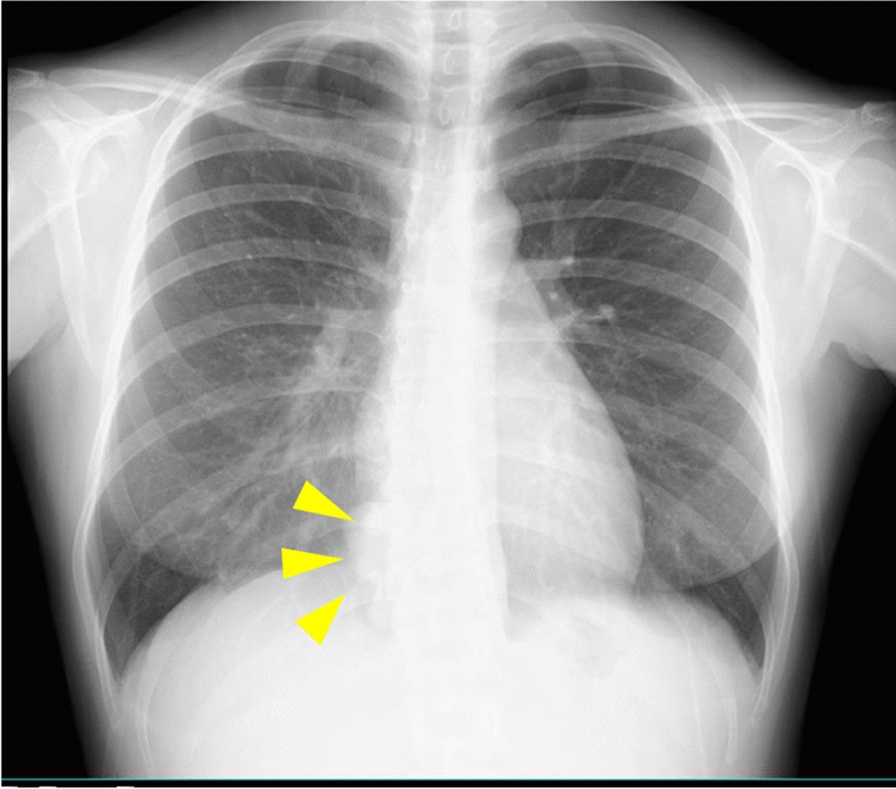
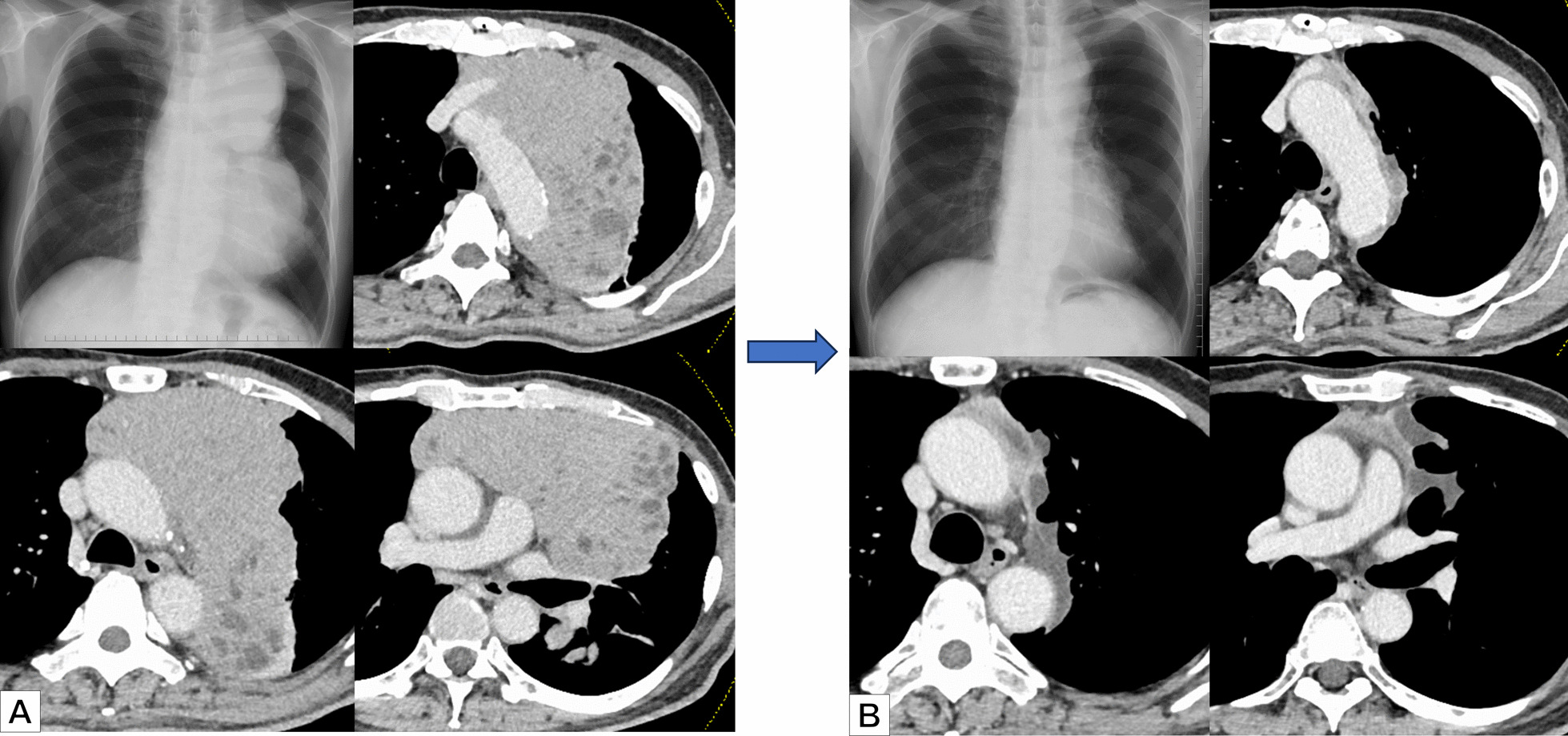
The patient had no symptoms and the tumor was incidentally detected on chest X-ray. Preoperative CT revealed that the tumor was in contact with the esophagus, and we initially suspected an esophageal submucosal tumor. Intraoperative examination showed that the tumor was located on the right side of the esophagus and was broad-based. Owing to the suspicion of a mediastinal tumor, complete tumor resection was performed under thoracoscopy. Twenty-two months after surgery, the patient is being followed up without recurrence. However, there is no established interval or duration of follow-up for completely resected CFTs of pleural origin.



留言 (0)