Multidisciplinary treatment of giant thymoma, paving the way to complete surgical resection: a case report
We report a case of a large thymoma occupying the left thoracic cavity. The thymoma presented surgical challenges, but was successfully treated with complete resection after preoperative induction chemotherapy. Complete resections of large or advanced thymomas may be difficult, and various treatment strategies have been reported. Multimodality therapy with induction chemotherapy followed by surgical resection is a widely accepted approach [1]. We previously achieved a high rate of complete resection and long-term survival with induction chemotherapy followed by surgery in patients with advanced or recurrent thymoma cases [2, 3]. Based on this experience, we treated the current case using a multidisciplinary approach and achieved a curative resection.
Although no standard chemotherapeutic regimen has been established for thymomas, several regimens have been introduced [3,4,5]. Yokoi et al. demonstrated that the CAMP chemotherapy regimen for patients with advanced-stage thymomas results in a response rate of 92.9%, 5- and 10-year overall survival rates of 80.7%, and no major adverse events except acceptable neutropenia [3]. Yokoi et al. concluded that CAMP therapy was highly effective for the treatment of advanced-stage thymomas. In the current case, the patient was treated with the CAMP regimen before surgery, demonstrating the feasibility and safety of this multidisciplinary treatment.
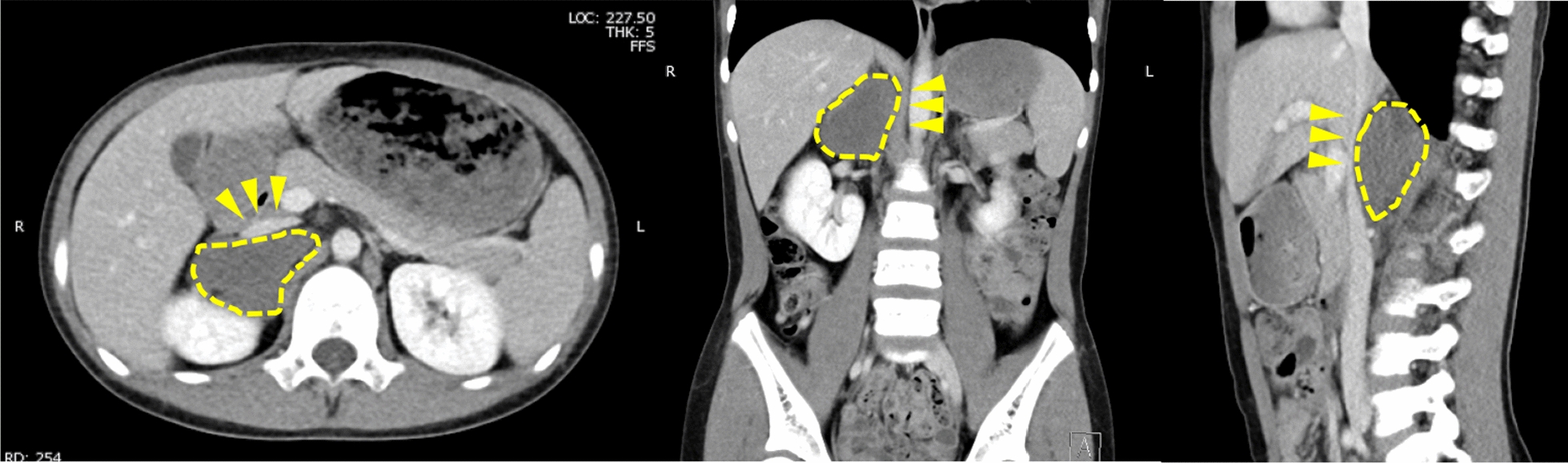
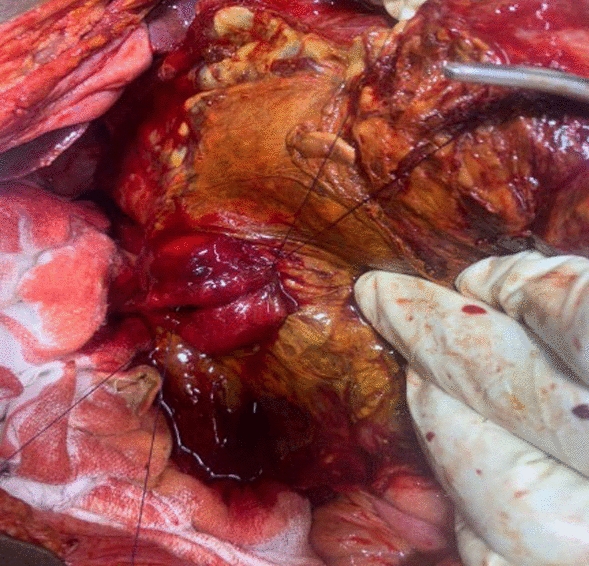
No standard surgical procedure for large or advanced-stage thymomas has been established. For curative complete resection in patients with thymomas invading adjacent structures, total thymectomy must be combined with resection of adjacent invaded structures to prevent postoperative local recurrence or pleural dissemination. In the current case, the thymoma was exceptionally large; CT showed the involvement of multiple adjacent organs, including the pericardium, pleura, phrenic nerve, and left upper lobe of the lung. Notably, the tumor extensively abutted the pleura, encompassing the mediastinal, parietal, and visceral pleura; the visceral pleura of the left lower lobe was also involved, raising concerns about pleural dissemination if these areas were not treated. To prevent pleural dissemination, complete resection would have entailed thymectomy with left total pleurectomy or extrapleural pneumonectomy. Considering the patient’s age and comorbidities, we performed total thymectomy, along with partial resections of the parietal, mediastinal and visceral pleura, pericardium, and left upper lobectomy. This approach achieved complete histological resection, mitigating the risk of recurrence.









留言 (0)