In this case, a patient who had PDAC with liver metastases at the initial diagnosis underwent conversion surgery after multidisciplinary treatment. To the authors' knowledge, this is the first report of a case in which conversion surgery was performed after olaparib therapy.
In the initial diagnosis and staging of PDAC, contrast-enhanced CT is generally the first step, and Gd-EOB-MRI and positron emission tomography (PET) -CT are performed as needed to scrutinize distant metastases [3]. We do not routinely perform Gd-EOB-MRI or PET–CT in all patients of PDAC. Even if we had, we do not know whether we would have detected the very small liver metastasis in this case, the so-called occult abdominal metastasis (OAM) [1]. After the first surgery in which micro liver metastases were discovered, the patient was followed up with MRI, which is suitable for identification of liver metastases. We have previously shown that PDAC patients with tumor diameter greater than 30 mm, CA19-9 greater than 150 IU/ml, and localization in the pancreatic body and tail are at greater risk of having OAM, and we recommended staging laparoscopy in such cases [13]. Although this patient did not undergo staging laparoscopy in favor of starting chemotherapy early, if it had been performed, it is possible that UR-M would have been diagnosed before the start of neoadjuvant treatment.
In 2020, Golan et al. published the results of a randomized, double-blind, phase 3 trial examining the efficacy of olaparib in patients with BRCA mutation-positive metastatic PDAC that had not progressed during first-line platinum-based chemotherapy [9]. The median progression-free survival (PFS), as a primary endpoint, was significantly longer in the olaparib group than in the placebo group (7.4 months vs. 3.8 months, respectively; hazard ratio for disease progression or death, 0.53; 95% confidence interval [CI], 0.35–0.82; P = 0.004). The trial also showed that the adverse effect profile of maintenance olaparib was similar to that observed in other tumor types. Health-related quality of life was preserved with olaparib.
Olaparib provides a survival benefit to patients with a germline BRCA mutation and metastatic PDAC that did not progress during platinum-based chemotherapy. When the chemotherapy regimen is changed from effective platinum-based therapy to maintenance olaparib with expected prolonged survival and less frequent adverse events, careful follow-up is required to monitor the patient for tumor progression.
The most frequently used platinum-based chemotherapy is FOLFIRINOX. In 2019, we reported the efficacy of SOXIRI therapy, which replaces 5-fluorouracil in FOLFIRINOX with S-1, in a two-center, single-arm, phase II trial for UR-M and locally advanced unresectable (UR-LA) PDAC [10]. The response rate, as a primary end point, was 22.8% (95% CI: 10.4–40.1); median overall survival (OS) was 17.7 months (95% CI: 9.8–22.0), and median PFS was 7.4 months (95% CI: 4.2–8.4). Thus, SOXIRI is considered a promising regimen in patients with unresectable PDAC. The patient described in this case report received SOXIRI therapy as platinum-based chemotherapy.
Surgical resection for liver-only synchronous metastases of PDAC, as in this case, remains controversial. Moreover, there are two major approaches, surgery-first and chemotherapy-first approaches, to the surgical resection of UR-M PDAC [8]. The former involves resection of a small number of distant organ metastases (oligometastasis) with the primary tumor without preoperative chemotherapy or after a short course of preoperative chemotherapy [14]. With the chemotherapy-first approach, after a period of multidisciplinary treatment, the primary tumor is resected in patients in whom distant metastases have disappeared or marked shrinkage is noted on imaging studies, so-called “conversion surgery” [7]. The OS of patients treated with the surgery-first approach was reported to range from 5.9 to 21.9 months [15,16,17,18,19,20,21,22,23,24,25,26]. On the other hand, the median OS was 34.1 to 56.0 months from the initiation of chemotherapy and 24.4 to 46.0 months after conversion surgery [18, 27, 28]. Thus, OS is apparently better with conversion surgery (chemotherapy-first approach) than with synchronous resection of the primary tumor and liver metastasis (surgery-first approach). Consequently, this patient was treated with the chemotherapy-first approach, and conversion surgery was performed successfully.
Our criteria for conversion surgery for UR-M PDAC were: anatomical resectability (absence of liver metastases in this patient), biological response to chemotherapy (CA19-9 in this patient), and good general condition of the patient. In addition, the appropriate timing for conversion surgery for initially UR-M PDAC has been still unclear. We do not currently define the duration of preoperative chemotherapy as an indication for conversion surgery. However, considering the results of previous studies, the duration of induction chemotherapy for decision-making regarding conversion surgery in patients with UR-M has been reported to be longer than at least 8–9 months for confirming disease progression (depending on tumor marker levels), resulting in favorable OS in patients with UR-M PDAC [29,30,31,32,33].
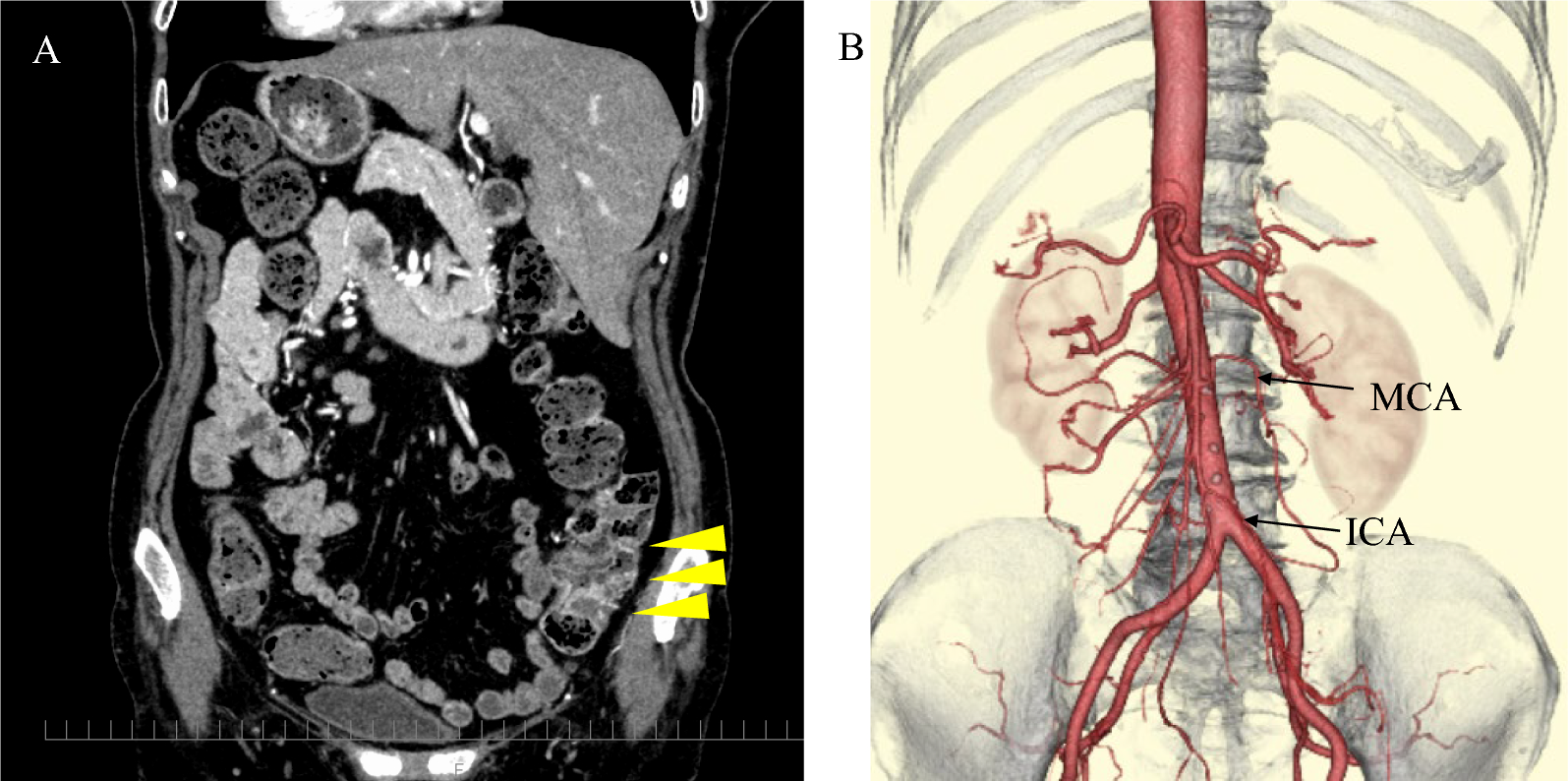
This patient had two liver nodules of the same nature, one of which was diagnosed as a liver metastasis at the first surgery (Fig. 3A, red circle). The other was diagnosed as not being a liver metastasis at the second surgery (Figs. 3A and 4A, yellow circle). It is possible that the other nodule (Figs. 3A and 4A, yellow circle) was not a liver metastasis from the beginning, but what is important is that there was no liver metastasis at the second surgery after 30 weeks of chemotherapy with SOXIRI and olaparib.
The significance of adjuvant chemotherapy after conversion surgery remains unclear. Whereas several previous studies of conversion surgery showed better patient survival with adjuvant therapy than without it [17, 29, 30], the appropriate regimen of adjuvant therapy after surgery for UR-M PDAC remains unknown [8]. There is no clear evidence to verify this. The standard regimen for postoperative adjuvant therapy for PDAC in Japan is S-1 for six months, but the clinical trials in which this was established did not include conversion surgery for UR-M PDAC [34]. It is unclear whether it is better to use the guideline-recommended regimen as adjuvant therapy or to again use the regimen that was effective for distant metastases in the preoperative treatment as adjuvant therapy. The patient in this report took olaparib for one year and had no recurrence. No evidence exists for the use of olaparib as adjuvant therapy, and it should be carefully studied in the future.



留言 (0)