In our study, 11 GPs (6 men, 5 women) of various age groups participated (Table 1).
Table 1 Socio-demographic data and information on residency program and employment statusThe presentation of the results follows the research questions, commencing with the role of palliative care (Q1), followed by an exploration of potential stressors (Q2), and coping mechanisms (Q3) and concluding with ACP (Q4).
Role of palliative care
The central objective of GPs in palliative care is to alleviate suffering and thus maintain quality of life (GP1; GP2; GP3; GP9). Palliative care holds a high to very high significance in the daily practice of GPs. It is perceived as an “inherent responsibility of general practice” (GP7) to accompany patients until the end of their lives. This perception was also reflected in their professional identity: GPs saw themselves as medical companions from childhood to death. The importance was not necessarily directly proportional to the actual level of palliative care provided: “For me, it is very important […]. But fortunately, it is a small percentage of patients” (GP10). The average number of patients with palliative care needs cared for per year showed a wide range. Most GPs (n = 8) stated that they treat up to 20 patients yearly, the maximum was over 60 patients (n = 1). The majority (10 out of 11) stated that between 0 and 20 patients with palliative care needs die in their care over the span of one year (Supplemental information 2).
Psychological and emotional stress experienced by GPsExternal stressorsJob content
For GPs, palliative care was considered a “routine aspect” (GP9), however, they reported a significant imbalance between effort and reimbursement (GP4; GP7; GP9). In general, GPs expressed openness to discussing death and related wishes with their patients. Some emphasized a moral obligation to address these topics (GP5), highlighting the ethical dimension involved. However, there were clear differences in how these discussions were initiated. While some GPs actively approached patients to discuss end-of-life care (GP3; GP4; GP7; GP9), the majority of them waited for patients to raise the topic. Many GPs appreciate when patients initiate these conversations, as it signals openness to the topic and provides a starting point. The most common triggers were critical health conditions, acute deteriorations, an unfavorable prognosis (GP2; GP4; GP7; GP9) or death in the patient’s social environment (GP9; GP10). The identified triggers also determine the primary target groups for these discussions: patients with palliative care needs, chronically ill individuals, older patients, and their respective relatives, along with those who actively approach GPs regardless of age or health status (GP2; GP3; GP7; GP8; GP9; GP10; GP11). Even with a specific trigger, GPs described that they sometimes hesitate to initiate discussions to avoid overwhelming patients. GPs also expressed concerns about potentially diminishing patients’ hope and will to live through discussions about death (GP4; GP6; GP8).
Central to these conversations is the understanding of patients’ preferences and wishes (GP1; GP3; GP5; GP7; GP8). This includes evaluating whether home care is feasible and if a move to a hospice is necessary and desired. The involvement of family members in end-of-life care and their alignment with the patients’ wishes is crucial (GP9). Requests for physician-assisted suicide were mentioned less frequently, and some GPs expressed relief about that: “many patients were so hopeless and deeply sad at the end, […] that they said ‘I would prefer to be dead right now.’ But I’m so glad that not a single person asked me if I could help them.” (GP10). When no specific wishes were documented, the presumed patient will has to be determined in acute situations. This can lead to challenging situations for all parties involved (GP7; GP8).
Work organization
GPs expressed a fundamental time constraint, noting that “the main part of (…) caring for dying patients is certainly a verbal one and that takes time. And the second point of course, is that these patients are often so ill that they need home visits” (GP1). A certain level of flexibility is often necessary because “palliative care is always something spontaneous and difficult to plan. I can’t really say I’ll keep ten to twelve free in my diary on Friday’ or something; that’s not really possible” (GP6). This time challenge becomes more pronounced when patients have not made any or only insufficient decisions regarding palliative care. GPs described advance care planning as time-consuming consultations to explain medical terms and treatment options (GP5; GP10). While justified given the gravity of the decisions, these lengthy discussions pose organizational challenges for GPs (GP1; GP2).
Work environment
Caring at home for patients with palliative care needs is commonly favored and often aligns with the patients’ wishes. The GPs named positive impacts of the familiar environment on the psychological well-being of patients (GP1). In certain situations, such as when the nursing care needs cannot be adequately met, GPs preferred hospice care. Some interviewees explicitly assessed any demand for round-the-clock availability as a burden (GP7; GP8).
The GPs mentioned the time constraints as the most prominent obstacle in the ambulatory setting (GP6). Another major disadvantage is that fewer resources are available compared to a hospital setting. Should instrumental examinations be necessary, this is associated with greater effort (GP1). The GPs addressed the lack of personal expertise and experience in approaching such challenges (GP1) (Also: Individual Precondition - Qualification). The work environment of GPs entails having limited on-site support, as exemplified by involving colleagues (GP6). The burden of bearing sole responsibility for decisions, without or with only limited chances for reassurance from colleagues or relatives, was perceived as challenging (GP9).
Legal context
The legal context played a prominent role in all the interviews. GPs’ explicit and implicit remarks showed that they perceived a lack of comprehensive legal protection when providing care to patients with palliative care needs, especially when it came to assisted suicide. This legal ambiguity has the potential to induce distress. Their own values and knowledge factor into this context (Individual Precondition). As these factors are difficult to sort from each other, they are presented together in this section. In the perception of the legal situation of physician-assisted suicide, the GPs’ assessments varied from “illegal” (GP3; GP11) to “allowed under certain conditions” (GP7). Their willingness to accommodate the request for physician-assisted suicide also varied from “strict refusal” (GP3; GP9; GP11) to “providing information about alternative options” (GP4) or to contact specific assisted dying associations (GP6). With a good and long doctor-patient-relationship, GPs were rather open to further measures: “I think it would very much depend on whether I have accompanied the patient until then and have such a, already such a relationship, you know. […] Then I believe, I could imagine it more easily.” (GP8). As inhibiting factors GPs cited personal values (GP3; GP9) and religious reasons: “we as humans [are] not empowered to end a life, you know. Even if the person wants or wishes it.” (GP11). GPs also stated role conflict, as to them physician-assisted suicide conflicted with the professional role of a GP (GP8; GP10). A significant barrier was the legal uncertainty among GPs (GP6; GP9): “And if the patient had then asked me to put an end to it, then […] I would actually have been afraid of losing my profession if I did something that is not currently allowed.” (GP10). However, the uncertainty also brought a temporarily relieving aspect: “I’m actually glad that it’s not legally clarified yet because I can hide behind it. If it were clarified, I would have to deal with it.” (GP9).
Social relationships
Several participants emphasized the pivotal role of emotional and social support, especially in palliative care (GP2; GP3; GP7; GP9; GP10). A stable relationship with the patients is beneficial: “knowing the entire […] environment of the patient. […] one can assess a bit where there are problems within the family or even in the household. […] So, I think that is an advantage that colleagues from other disciplines cannot have because they are not so on-site. And often, they don’t know the patients for as long.” (GP3). Conversely, palliative care poses a significant challenge when a stable relationship has not yet been established (GP2; GP7). The sense of security conveyed to patients with an established trust was seen as a factor that strengthens GPs in their work: “Because I simply wanted to be there for my patients when they go. Because they have a bit more security there. After all, those were unfamiliar doctors [in the hospital]. […] when your own GP stands beside and essentially approves of what is happening, that’s something completely different.” (GP10). When relatives or close individuals are involved in palliative care, the GPs must gain their trust as well (GP2; GP9). Gaining trust often requires (time-)intensive and emotionally charged conversations (GP5; GP6). Nevertheless, GPs considered involving relatives closely and early as an important aspect (GP9; GP11) as relatives can also reduce the workload for GPs by being guided, for example, in the administration of medications (GP11).
Societal conditions
The societal discourse surrounding the topic of mortality is perceived as challenging. Death is “naturally tabooed in society” (GP11) less so in the professional context (GP8). The societal taboo around deterred GPs from initiating these conversations (GP11). GPs even feared societal condemnation as “involuntary angels of death” (GP7) if they fulfill the requests for physician-assisted suicide. At the same time, there is a growing societal acknowledgment of palliative medical practices as supportive. Particularly, the gratitude expressed by those immediately affected was considered as “justifying the effort” (GP9).
Individual preconditionsPersonal attitude
Although palliative care is an inherent responsibility, death itself played a rather subordinate role in the everyday thoughts of the GPs surveyed. In the short survey, 72.7% stated that they do not think about the death of themselves, loved ones, or patients more than once a day (Table 2). There was also predominantly little fear of contact with death. Despite the GPs’ reservations about physician-assisted suicide, they understood patients’ desire for medical support about a self-determined death (GP6; GP7; GP10, Table 2). In the survey, six GPs agreed that everyone should have the freedom to decide for themselves how they want to die.
Table 2 Selection of relevant questions regarding the GPs’ attitude towards deathGPs found it challenging when patient or family preferences did not align with their assessment (GP8; GP11). This often occurred when family members sought maximum care, seen by GPs as an unnecessary burden.
Qualification
The majority of GPs (10 out of 11) felt emotionally prepared for the care of patients with palliative care needs. The level of experience in the sample was very heterogeneous. Some GPs (n = 4) stated in the interview that they had not attended any further training. Mostly these GPs (but not exclusively) reported a lack of knowledge (GP8; GP11). For the other GPs, the further training varied between self-study (n = 1), seminars (n = 2) and additional training in palliative medicine (n = 4). Despite GPs expressing a high level of clinical experience, they wanted more training, as palliative care “is somewhat overlooked in training despite its elevated priority” (GP3). The perceived lack of qualification increases the risk of a stress reaction. No predominant motivations for pursuing more extensive training could be discerned within the sample.
When assessing the GPs’ concerns about making mistakes in connection with palliative care, the overall mood was fairly balanced, with a slight tendency towards fear of making mistakes (Table 3).
Table 3 Selection of relevant questions regarding the GPs’ qualificationThere were discrepancies between the quantitative and qualitative data regarding communicative and psychosocial skills. In the quantitative data, the GPs predominantly expressed positivity regarding their communicative competencies. Specifically, 63.64% (n = 7) asserted competence in attentive listening to individuals in the terminal phase, and 72.73% (n = 8) expressed confidence in being able to have conversations with the dying. Communicating unfavorable prognoses presented only for 18.19% (n = 2) of GPs a specific challenge. However, in the interviews, GPs described a deficiency in training related to communication skills and offering psychological support to patients and their families (GP8; GP10; GP11) as “no one teaches you how to conduct conversations“ (GP11).
Emotions
GPs described palliative care as highly emotional. Some GPs mentioned that palliative care treatment pushes them to their emotional limits (GP9; GP11). Negative emotions described were a certain sense of discomfort, frustration, and helplessness (GP2; GP5; GP9; GP10). They perceived a younger age of patients and parenthood of younger children as emotionally more challenging (GP5; GP7; GP8). When they could identify themselves with the patients (e.g., through similar age or similar family situations), emotional involvement increased as the GPs were confronted by their own mortality (GP4; GP7; GP9). It is also challenging when patients or their families react defensively or deny the overall situation (GP5; GP6; GP11).
The lack of social support for the dying (e.g. during the COVID-19 pandemic) triggered negative emotions (GP11). GPs reported that the grief of the families or the fear of the patients also affects them (GP2). This is aggravated by a “feeling of guilt” if the care “simply did not go well and it could have been better” (GP4).
However, palliative care can also evoke positive emotions, mostly described when patients are well-cared for in all four aspects of palliative medicine (physical, psychological, social, and spiritual). The social support provided by family members is particularly emphasized in this regard (GP2; GP10). GPs described gratitude from patients and family members, leading to a nonspecific positive feeling (GP6; GP7). In general, positive emotions were typically triggered when GPs felt they have achieved the best possible care for patients.
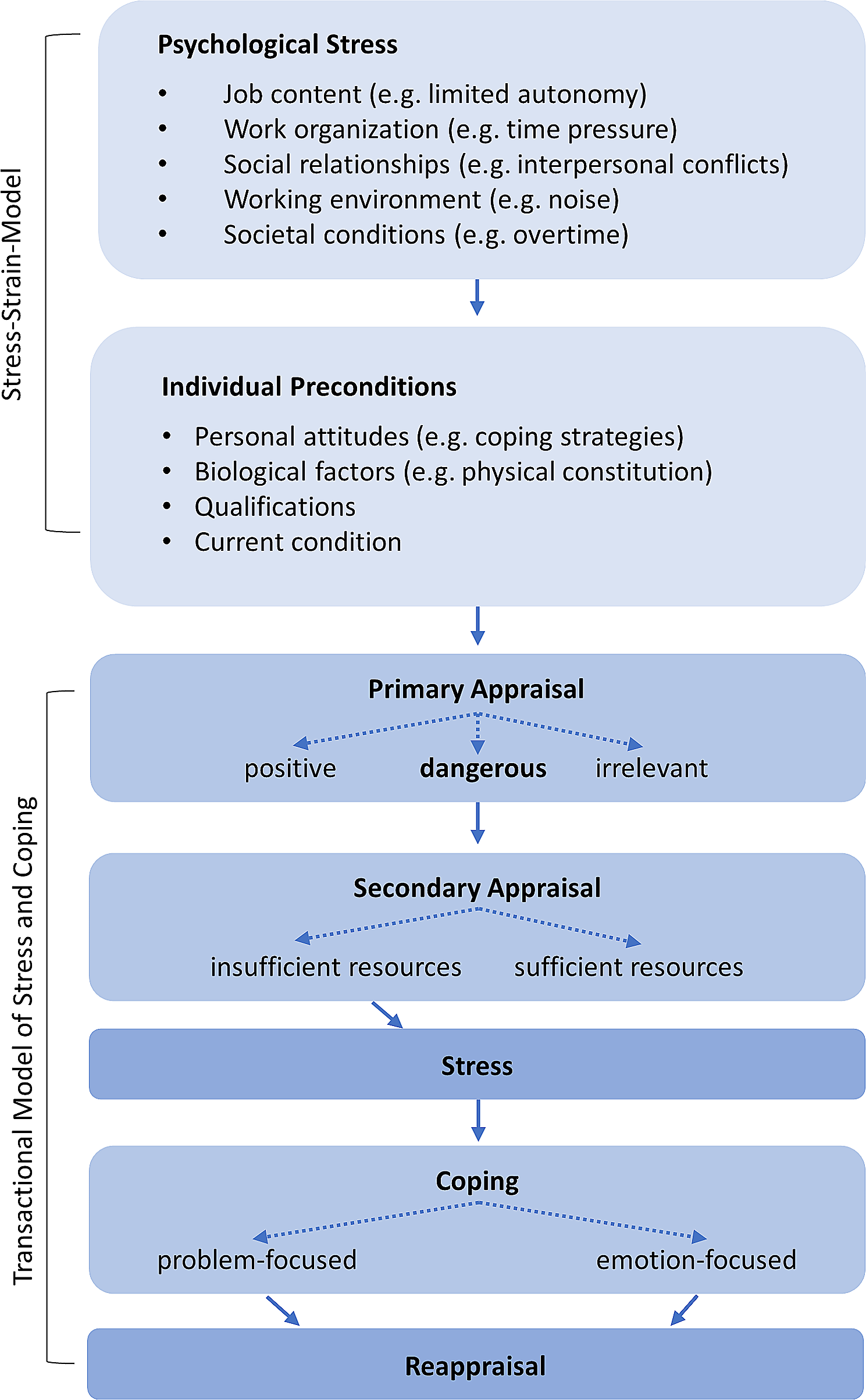
Dealing with stressorsPrimary appraisal
Some GPs rated palliative care as neither a positive nor a negative stimulus. If the external stimuli were assessed directly as “irrelevant”, active processing and dealing with any emotions was not necessary for the respective GPs. Some GPs appraised stimuli from palliative care activities as positive and enriching (GP3; GP6; GP7). In this case, no coping strategy was necessary as there was no negative stimulus to navigate. However, contrasting opinions also emerged, indicating that certain GPs regarded (parts of) palliative care as a potentially distressing stimulus, requiring coping strategies for the situation.
Secondary appraisal
The secondary evaluation occurs when a stimulus is initially perceived as potentially threatening. GPs identified high resilience and personal spirituality as protective elements for compensating for initially threatening stimuli (GP4; GP6; GP7; GP8; GP10). The interconnectedness of life and death was acknowledged, with the understanding that “death [is] a part of our lives” (GP6). This perspective helped them to cope with stressful situations. Addressing one’s mortality and thoughts about dying also facilitated communication with patients (GP4). Additionally, the importance of maintaining a good work-life balance was emphasized for the ability to accumulate and utilize sufficient personal resources (GP4; GP6). The GPs described a kind of emotional balancing. As positive emotions dominate in palliative care, they were able to compensate for the negative feelings (GP7).
Coping
If negative stressors cannot be sufficiently compensated for by protective factors, a coping mechanism becomes necessary. Problem-focused and emotion-focused coping strategies were evident in the GPs’ statements. However, a few of the GPs stated that they did not have a specific coping strategy.
Problem-focused coping
Some GPs described that they either proactively avoid situations that could lead to negative stressors or, at the very least, attempt to delegate a significant portion of the responsibility to other colleagues or external teams (such as SAPCT teams) (GP5; GP8, GP9). Another way to engage in problem-focused coping is through an organized work routine. Measures perceived as supportive include scheduling and incorporating buffer times (GP10) and conducting in-depth conversations to address the concerns of patients and their families. Establishing a 24-hour telephone availability for patients with palliative care needs and their families was discussed rather differently, either as supportive or as a further stressor (GP2; GP9). SAPCT teams were often cited as the primary source for both temporal and professional relief, especially as they are available 24 h a day (GP1; GP4; GP5; GP8; GP9; GP11). The lack of personal resources can thus be compensated for through interprofessional collaboration (GP5; GP7; GP9; GP11). Simultaneously, collaboration always involves an interface. Therefore, effective communication is essential, and its absence was otherwise perceived as a burden (GP7).
Emotion-focused coping
The spectrum of emotion-focused coping is diverse, individual methods range from practicing autogenic training (GP9) and engaging in sports (GP4) to having intensive conversations. Balint groups or colleagues in the practice were emphasized as helpful: “One often discusses this with colleagues. I find that always super important, yes. […] That is actually the most effective coping measure for me.” (GP5). GPs only occasionally mentioned conversations with family and friends as a personal relief (GP7; GP8). Individual reflection and recapitulation of situations were also described as coping strategies (GP2; GP5). GPs mentally went through the treatment situations, evaluating where things went well and identifying areas for potential improvement. The consensus between the measures taken and the wishes and needs of the patients is particularly relieving in retrospect.
Occasionally, GPs kept their thoughts and emotions at a distance, leading to expressions like “to a certain extent, I don’t care” (GP1). For some, the distancing is the only way to fulfill the role as GP and to be able to handle the emotions of patients and their families.
ACP in primary care
Except for three GPs (GP1; GP3; GP7), the concept of ACP was unfamiliar to German GPs. The responses to ACP, however, were largely positive. Particularly, the initiation of discussions can be made easier by a structured program like ACP (GP2; GP9). Once the conversation has started, further discussions become easier: “It’s like pushing a car. It requires a lot of effort to get it moving initially, but once it’s in motion, it’s relatively easy to push it a bit faster.” (GP9).
The GPs perceived the concept as more detailed and specific than an advance directive, yet they believed that it does not guarantee the discussion of the actual health conditions that may occur in advance (GP4). They emphasized the time problem again (GP11), making it impractical to offer ACP to all patients (GP8). The most frequently cited reason for individual relief for GPs was the existence of a specific action plan in the event that the respective patients become incapable of making decisions (GP2; GP6; GP7; GP8; GP10; GP11), especially in acute situations (GP8). GPs also mentioned personal protection against accusations from relatives (GP7). They evaluated ACP as emotionally challenging, especially when measures need to be withheld that are not in line with their preferences (GP1; GP8). Additionally, limited relief options were perceived when the treating GPs are not part of the advance planning process (GP1).




留言 (0)