In this cohort study the relationships between the Nascher score, which has been developed and used for routine purpose since 2007, and the various outcome parameters of medical needs and risk of death were analyzed. Based on the findings of a first analysis with the original scoring system, an alternative scoring system for the Nascher score was established. There was a significant correlation between the Nascher score upon admission to the nursing hospital and the number of medication changes per year, the number of ward doctor documentations per week, and the number of episodes treated with antibiotics per year. Furthermore, a higher Nascher score significantly predicted a higher mortality risk, even given age, sex, and level of care.
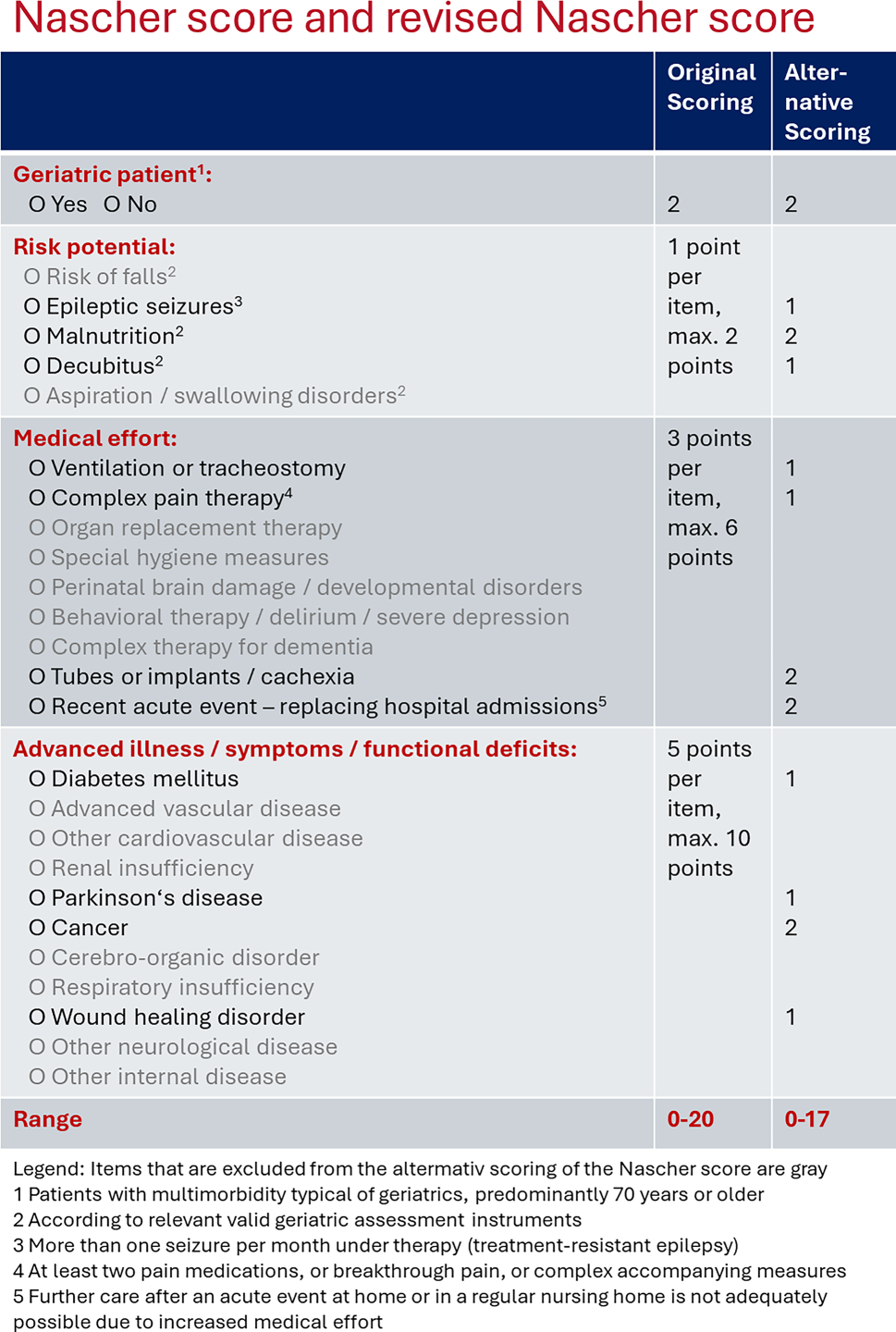
Both the Nascher score and the revised Nascher score showed very good predictive power for medical needs, with the revised Nascher score performing slightly better. Furthermore, the revised Nascher score has several advantages over the original version: (1) fewer parameters are required to perform the scoring (12 vs. 26 items) and therefore it is significantly less time-consuming and (2) the revised Nascher score is normally distributed. This implies the advantage of applying parametric statistical methods, which are more powerful and versatile than the non-parametric alternatives required for skewed data. This enhances the reliability and validity of the assessment tool by enabling precise comparisons across different groups and time points. Moreover, a normal distribution ensures that extreme scores are proportionately represented, preventing the distortion of results that could lead to inaccurate interpretation. For instance, the use of normally distributed scores in clinical assessments has been shown to improve the precision of diagnostic tools and the effectiveness of therapeutic interventions [10].
Surprisingly, to date the assessment of medical needs has received little attention in geriatric assessment. While future medical care needs are usually not specifically addressed in routine geriatric assessments, they often include elements that indirectly address future health. This includes evaluating risk factors for falls, frailty, or common geriatric conditions, which then individually and through their interaction determine the medical needs [11]. Therefore, the Nascher score could be viewed as a shortcut to assess medical expenditure. Furthermore, planning for future medical needs is often addressed through other services and discussions, such as advanced care planning, palliative care consultation, and long-term care planning [12]. The Nascher score could help with making decisions about nursing and medical care pathways, especially with respect to medical care, including whether the presence of physicians is needed around the clock or not.
Some items of the Nascher score were particularly strongly associated with future medical needs, i.e., designation as geriatric patient, malnutrition, presence of tubes, implants, or cachexia, recent acute events, and malignancies. Malnutrition is, along with sarcopenia and chronic inflammation, the most important factor involved in the development of frailty. Furthermore, frailty is a geriatric syndrome that predicts many negative outcomes [13]. In addition, malnutrition is often the result of many chronic diseases that are consumptive and involve loss of appetite, difficulty chewing or swallowing, or malabsorption [14], and malnutrition predicts many adverse health outcomes [15]. Very often cachexia is a result of malnutrition and requires oral supplementation or enteral nutrition [16]. It is therefore not surprising that malnutrition and also the presence of tubes, implants, or cachexia predict medical needs so strongly. Cancer was also a diagnosis that very strongly predicted medical needs. Medical needs in patients, even after acute cancer treatment, remain high and include care for long-term side effects and complications of surgery, chemotherapy, radiotherapy and immunotherapy, and life-long therapies such as hormone replacement, but also surveillance for recurrence and secondary cancers, chronic health conditions, and mental and psychological support. These are also reasons why patients with cancer significantly benefit from routine geriatric assessments [17, 18].
To evaluate the Nascher score, two apparently very different outcome clusters were used: medical effort and death; however, the time just before death is often a medically very complex and intensive time [19]. This was also shown by a recent analysis with data from the same cohort [20]. Therefore, it is not surprising that the Nascher score results are similar with respect to both outcome clusters. About half of the patients included in the study died during the observation period, a median of 3 months after admission.
Notably, the level of nursing care at admission was not a predictor of death, in contrast to the Nascher score. This underlines that in geriatric care medical care needs and nursing care needs are two distinct concepts, each addressing different aspects of an older adult’s health. An integrative approach is essential where medical care and nursing care complement each other to address the comprehensive needs of older adults [21, 22]. In this sense, applying the Nascher score could very well complement assessing nursing care needs in terms of medical care needs.
Assessing future medical needs in geriatric patients is important for optimizing patient outcomes and resource allocation. Geriatric patients often present with complex, multimorbid conditions that require ongoing, multidimensional assessments and individualized interdisciplinary care plans to be managed effectively [23, 24]. Medical staff in long-term care facilities are uniquely positioned to implement and monitor health conditions, enabling a proactive approach to healthcare that is responsive to the nuanced needs of the residents. This continuous assessment framework supports the integration of preventive strategies, personalized treatment plans, and coordinated care efforts, thereby improving overall health outcomes and operational efficiency within these facilities [25].
The strength of this study is that it is the first analysis of the predictive power of an instrument that has been used for many years to assess medical needs in geriatric long-term care nursing hospital residents. This was analyzed using a cohort of all the people who were admitted to the nursing hospitals of Haus der Barmherzigkeit over a 2-year period, with an observation period of up to 2.5 years. Conscientious and complete electronic documentation over many years was a prerequisite to make this analysis possible. A possible limitation inherent in the retrospective nature of this study is that the outcome parameters were recorded for the continuous documentation of the medical needs and not primarily with the intention of conducting a scientific study. To date, the Nascher score has only been used in geriatric long-term care hospitals in two locations. The analysis was performed with a limited sample size of 396 subjects. Therefore, the generalizability to other settings is limited. Another limitation is that no data for sensitivity or specificity are yet available, and no comparisons with other clinical scores were performed. In the future, the Nascher score could be further developed, including possible changes to the categorization, application of the Nascher score in other healthcare facilities, and observations over a longer period of time.
In conclusion, it can be said that the Nascher score and even more so the revised Nascher score are well suited to predict the various parameters of future medical needs. Furthermore, a higher Nascher score is associated with a higher mortality risk. The Nascher score can be used to determine the adequate level of medical care in geriatric patients by discriminating between those who require more or less medical care and can therefore be added to routine evaluation of nursing needs and geriatric assessment.

留言 (0)