In comparison to the 25–46% [5,6,7] of overall patients with low or marginal HL mentioned in previous studies, patients in this outpatient setting achieved far better results. It can be argued that patients who explicitly visit the trauma outpatient department have a certain level of health understanding. This could be explained by the distinct separation of the trauma department and early triage in German-speaking countries of physical trauma patients from other general emergency patients.
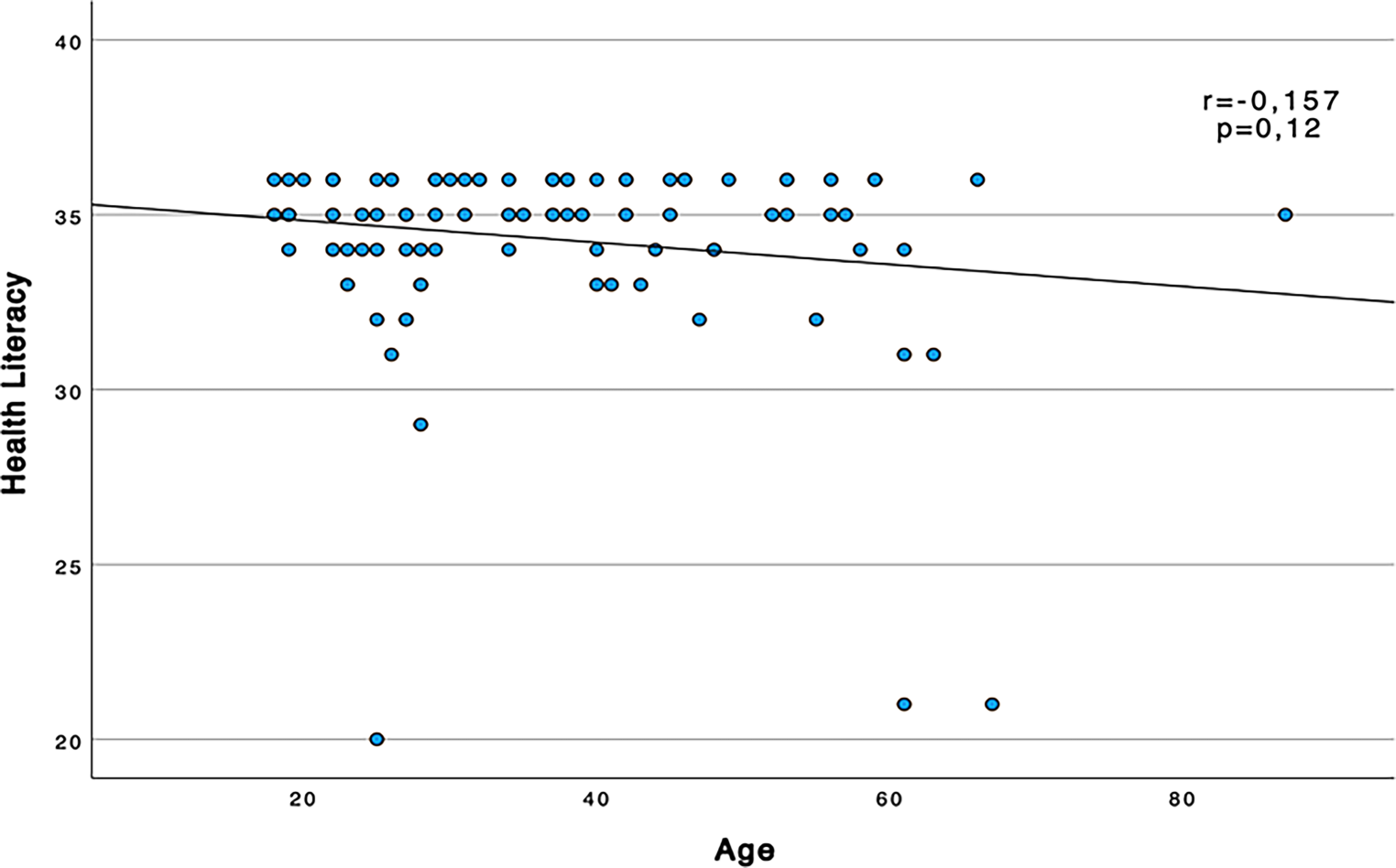
The 100 randomly selected patients showed considerable diversity in age and educational level. Based on the data of this study, there is no statistical significance in the correlation between HL and age. Nevertheless, as shown in the figure (Fig. 1), we did observe a tendency for HL to decrease with age, which has already been described in the literature [9]. Due to the sociodemographic trends of an aging society, this may indicate that in the future an increasing number of older people with low HL will emerge. Although not statistically significant, lower HL was found in patients with lower levels of education. This has also been shown in several previous studies [15].
Moreover, no significant difference in HL between patients born in German-speaking countries and patients with another mother tongue was apparent in this cohort.
Following the results of this study with the German S‑TOFHLA, there is no reason to believe that HL in trauma patients is severely impaired; however, due to the separation of injuries and emergencies in the Austrian triage system, no information can be provided regarding other emergencies. Furthermore, the instrument used shows ceiling effects, so that results have to be interpreted carefully.
The educational data from Statistics Austria showed that in 2020, 50.5% of the Austrian population had no high school diploma, 30.4% had a high school diploma and 19.1% had a higher educational qualification. Compared to our patient population, there were many more patients with a higher level of education, which could also explain the ceiling effect [16].
Although the German version of the S‑TOFHLA has been validated, the question still arises as to whether the questionnaire itself or the scoring system should be re-evaluated [14].
The S‑TOFHLA in this sample had a marked ceiling effect, which reduces or even removes its ability to discriminate between groups that may indeed differ in HL. An indication of this failure of S‑TOFHLA was found by re-evaluating the findings after dichotomizing the score at a value of 32, which resulted in significant differences for educational and age groups.
We additionally assessed the width of the S‑TOFHLA subgroups as too broad and therefore lacking informative value. By narrowing down the threshold and including the former “marginal” evaluation within the “inadequate” group, we have been able to attain significant differences; however, we are convinced that in larger study groups significant results could be possible even with 3 subgroups (adequate, marginal, and inadequate). Alternatively, the patient collective with a similar distribution of the level of education as in the data from Statistics Austria would be more conclusive. While an overall outstanding HL apprehension of outpatient physical trauma patients is a desirable outcome welcomed by medical staff, overestimation of general understanding could lead to potential risks.
In contrast to these findings, a systematic review of studies applying the S‑TOFHLA in the USA found that 10.5–32% of patients showed marginal or inadequate HL [7].
Interestingly, in Connor et al.’s (2013) Swiss validation study on the German S‑TOFHLA version, a total of 233 participants (93.6%) showed adequate HL. Only 7 participants (2.8%) showed a marginal score, and 9 (3.6%) presented an inadequate score. These results, although not acquired in an emergency department setting, are in good agreement with our findings [14].
This could be interpreted as an overall higher score using the German S‑TOFHLA. Whether those test results are generated due to an easier test version or indeed due to higher skills, shown e.g., in reading comprehension or HL, is yet to be determined and would require more follow-up studies.
Although attempts to validate the German version of the S‑TOFHLA have been undertaken [14], we still advocate revising this instrument due to its inefficient discriminatory power.
Concerning our initial results following the validated HL questionnaire scoring system 2 of the 3 patients considered with a marginal result were older than 60 years, further contributing to the discussion of whether the current evaluation displays a reliable measurement tool. The third low scorer came from a non-German speaking country and although of higher education was not sufficiently fluent in German to score high in the S‑TOFHLA. Hence, the overall poor HL could be significantly higher than that evaluated; however, it is unclear to what extent the data collected in this study are compromised by this language issue.
Providing an additional validated section, where potential poor results can be further attributed to either language or understanding could supply valuable insights and help improve the delivery of medical information.
Facing patients with an overall inadequate understanding, simplification of complex medical terminology as well as avoidance of technical terms should be thoroughly practiced.
Moreover, incorporation of visual aids such as diagrams, charts, and illustrations can be utilized to supplement written or spoken information. Through this visual assistance, complex concepts can be conveyed more effectively for individuals with limited literacy skills or language proficiency [17].
When engaging in a conversation the provider of medical information should ensure and promote two-way communication to ensure comprehension and address any questions or concerns patients may have. Compliant patients can be frequently asked to repeat or summarize certain aspects throughout the conversation. Especially with multilayered, codependent, and more complex information, this principle can ensure the comprehension of each step [17].
A cultural component is also to be considered regarding communication with patients. It is crucial to recognize cultural differences in communication styles, beliefs, and practices when delivering healthcare information and to tailor communication approaches to resonate with diverse cultural backgrounds [18].
If the insufficient understanding is due to a pronounced language barrier, brochures and pamphlets should always be provided in multiple languages to accommodate individuals who may not be fluent in the local language [19]. Additionally, interpretation services such as in-house interpreters or online language tools for real-time communication should be available to avoid misunderstandings [20, 21].
Due to the ceiling effect, which was already shown in the German-speaking collective of Connor et al. (2013) and is reproduced in this study, the question was raised, whether the German S‑TOFHLA is accurately validated [14]. This could mean that the German S‑TOFHLA needs a modification, either in its cut-off values or in the translation of the questions from the original English S‑TOFHLA. Based on the study design this statement can currently be applied to outpatient physical trauma patients only; however, it must also be taken into consideration that the concept of HL looks different in various parts of the world. Before implementing and using tools such as the S‑TOFHLA, the requirements for HL itself as well as the resulting adequate communication between healthcare provider and patient should ideally be analyzed.
While Özdemir et al. (2020) considered their study population in the emergency department to have an overall lower HL than the average population [1], we cannot support this assumption based on our results or missing reference values from other local medical departments. We found a significantly lower percentage of patients with marginal or inadequate HL, potentially caused by the instrument used. Even after the re-evaluation of our results using the modified scoring system, we observed a greater overall understanding of medical information in our study.
While the consequences of low HL may be limited in the outpatient setting, its impact may be of a much greater scale in the inpatient setting caused by the greater amount of medical healthcare information and the requirement for better understanding, compliance, and following more complex instructions. In this respect, there are few to no studies regarding physical trauma patients.
The questionnaire study can only provide a momentary perspective at the time of the outpatient presentation. The extent to which patients now follow the medical instructions and the posttreatment regimen cannot be determined on the basis of the evaluations of this study. To obtain the best possible results, a prospective study could be conducted in which not only questionnaires such as the S‑TOFHLA are completed by patients but also correlations are made with compliance in the posttreatment regimen. This could provide more concrete information about HL in outpatient physical trauma patients.
Limitations
Overall, the system-based sorting of physical trauma patients could impose a certain bias, as a basic level of HL can be expected if a patient knows which department to visit based on their medical condition. Another limitation is the fact that only data from complete questionnaires were analyzed. By handing the questionnaires out personally, the attending resident may have inflicted a personal bias on the composition of the study group, based on the impression, of whether a patient would complete the S‑TOFHLA.

留言 (0)