Fractures at levels T3 and T4 appear to be at higher risk to cause concomitant esophageal injuries than vertebral fractures at other segments, considering that most cases in the literature so far reported on vertebral fractures at this level [2, 4,5,6,7,8,9]. So far, 11 case reports have been published on vertebral fracture following trauma with associated esophageal injury (Table 1; [2,3,4,5,6,7,8,9, 11,12,13]). All but one [13] reported on distraction and/or translation injuries, whereas in our study, a split fracture was diagnosed on CT scan. Notably, as no MRI images were carried out owing to the patient’s critical general condition, the presence of a more unstable fracture type cannot be ruled out with certainty. Although high-energy driving accidents seem to be the prevailing cause of esophageal injury secondary to vertebral fractures [2,3,4,5,6,7, 9, 11, 13], our patient had experienced relatively mild trauma. Of note, in these cases, degenerative changes (e.g., due to ankylosing spondylitis) of the vertebral column are usually present [8, 12], similar to our patient’s DISH. Additional features potentially associated with esophageal injury secondary to vertebral fracture have not been described so far.
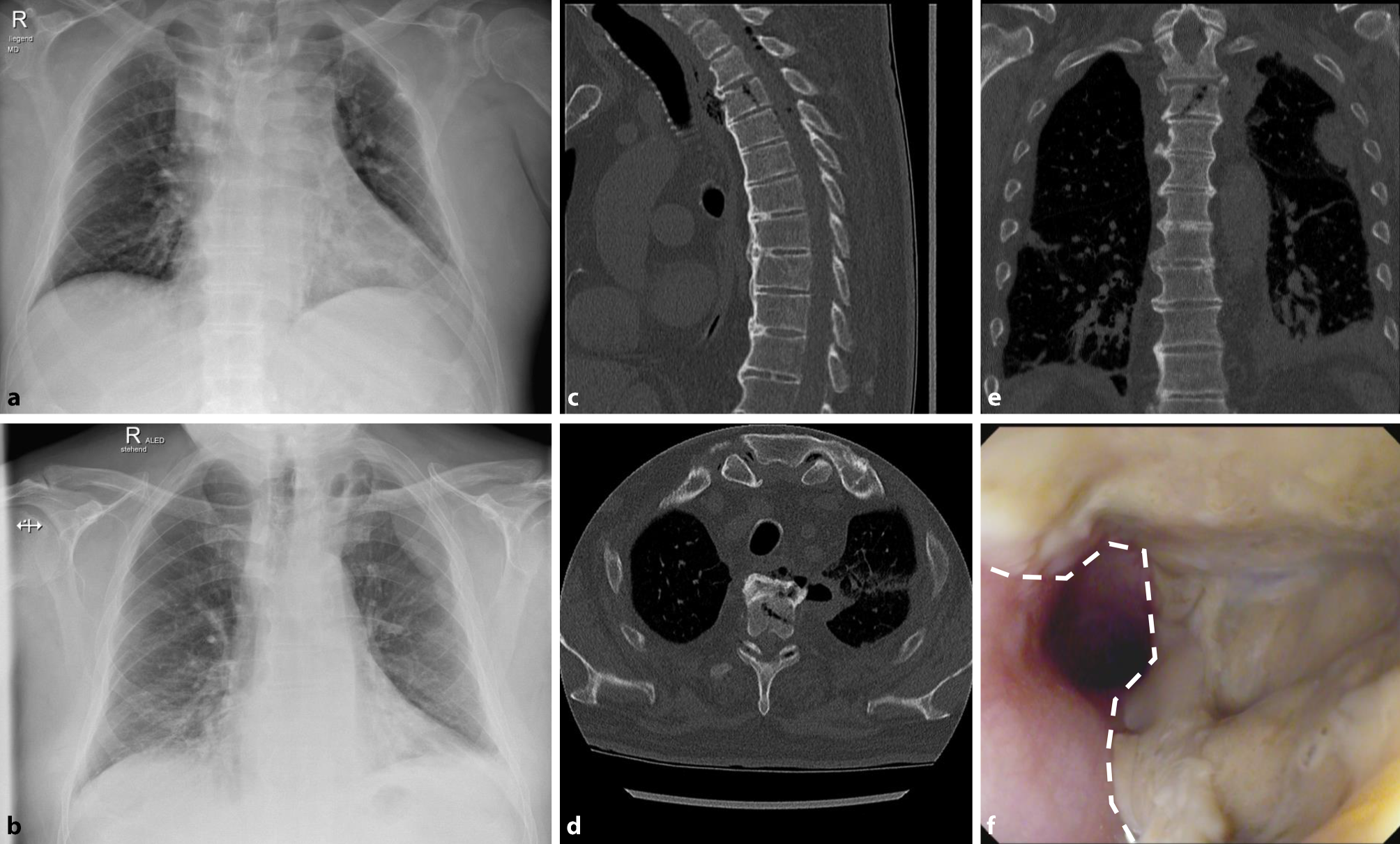
Table 1 Case list of esophageal injury secondary to vertebral fractures published in literatureAs previously reported [2, 3, 7, 8, 11,12,13] symptoms indicative of esophageal injury, such as dysphagia or vomiting were lacking in our patient at initial presentation. Supposedly, the accompanying rib fracture may have masked pain actually related to the vertebral fracture, wherefore further diagnostic work-up despite thoracic X‑ray showing a reasonable injury was omitted. Unsurprisingly, pneumonia was suspected when the patient presented 5 days after trauma with septicemia. Thoracic CT scan did not only reveal signs of mediastinitis with peri-esophageal air entrapment, but also trapped air within the spinal canal, a feature indicative of esophageal rupture [4]. Due to the rarity of esophageal perforation secondary to vertebral fracture, and either masking by other injuries following high-energy trauma (e.g., long bone fractures, pneumothorax, brain injury) or low-energy trauma rendering severe internal organ injuries unlikely, the diagnosis was likewise delayed in most previous cases [2, 3, 5, 7, 11,12,13].
In line with other reports [3,4,5, 9] multidisciplinary management including fast and extensive surgical debridement, esophagectomy, i.v. antibiotic therapy, and secondary reconstruction via gastric pull-up was essential to save the patient’s life. Herein, antibiotic therapy was discontinued after 12 days due to decreasing inflammatory parameters. In retrospect, this can be seen critically given the anatomical proximity of the esophageal perforation and vertebral fracture, and thus a high risk for subsequent spondylitis. Nevertheless, apart from repetitive endoscopic dilations due to esophageal constrictions, the patient did not develop any further complications up to the latest clinical visit.

留言 (0)