This study examined the impact of cycloplegia on the repeatability and agreement of autorefraction, keratometry, and axial length measurements in young individuals. Cycloplegia enhances autorefraction repeatability and modestly improves AL repeatability. Autorefraction repeatability is influenced by refractive error, with myopic individuals exhibiting superior repeatability compared to hyperopes. Additionally, cycloplegia induces a more positive SE, although the pre- and post-cycloplegia SE difference varies based on refractive error.
Autorefraction
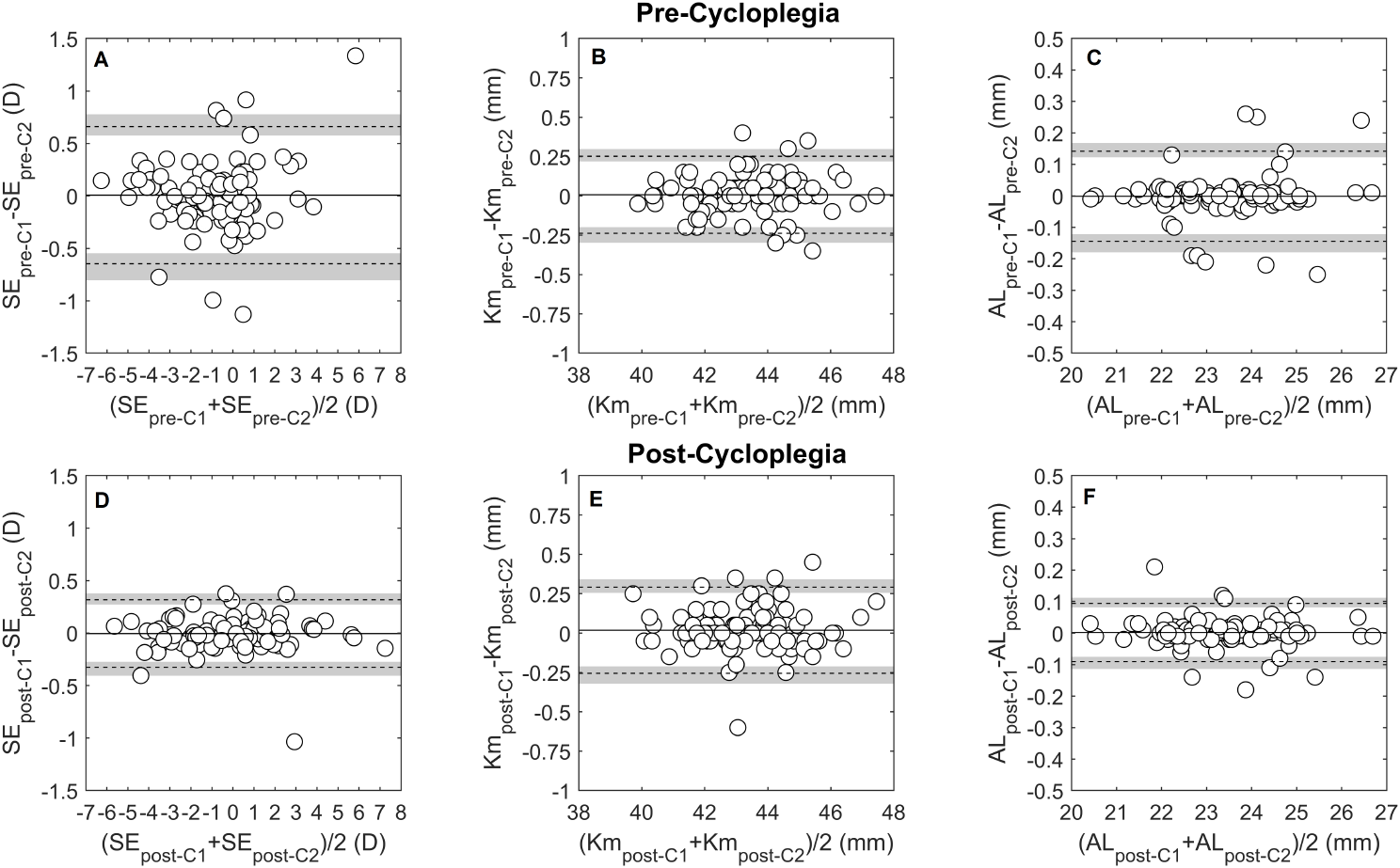
Cycloplegia significantly enhanced SE repeatability, reducing it from 0.65 to 0.31D across the entire sample, resulting in an increase in eyes with differences of up to ± 0.25 D from 73 to 93%. Among refractive error groups, emmetropes and myopes exhibited similar TRTs of ∼0.50 D, while hyperopes demonstrated higher TRT of ∼0.90 D. Despite cycloplegia halving the repeatability range to about 0.25 D, hyperopes still showed larger differences (TRT = 0.44 D) between repeated measurements, highlighting limited repeatability of the Myopia Master in hyperopic eyes. This suggests a potential necessity for additional cycloplegia (longer and higher dosage) in hyperopes for consistent autorefraction measurements.
The Myopia Master’s non-cycloplegic SE repeatability aligns with other autorefractors. For instance, Padhy et al. in a wide age-range group reported TRT values varying from 0.50 D (wavefront-based autorefractor) to 0.81D (table-top autorefractor). They linked the autorefraction repeatability to the autorefractor’s working principle [8]. Venkataraman et al. reported similar results, emphasizing enhanced repeatability in autorefractors with integrated defocusing systems [9]. In paediatric population, where high levels of accommodation are common, autorefraction repeatability may further depend on the type of autorefractor. Dahlmann-Noor et al. reported a TRT of 0.63D for a photorefraction system measuring distance at 1.0 m [17], compared to 1.57D with a hand-held system that elicits more proximal accommodation [18].
Rosenfield and Ciufreda observed improved SE repeatability following cycloplegia in a small paediatric group, particularly in instruments eliciting higher proximal accommodation. Post-cycloplegia repeatability ranged from 0.27D (retinoscopy) to 0.84D (hand-held autorefractor), in agreement with the present findings [19]. Similarly, Rauscher et al. utilizing a table-top wavefront-based autorefractometer, reported a reduction from 1.49D pre-cycloplegia to 0.64 D in the 95% interval of accommodative variations during sequential readings [20].
Cycloplegic refraction introduced a SE bias of + 0.79 D compared to non-cycloplegic refraction, attributed to a reduction in crystalline lens power [11]. In a meta-analysis, Wilson et al. observed that non-cycloplegic SE closely approximated cycloplegic SE when employing a photorefraction technique (Pluxoptix). However, hand-held and table-top autorefractors tended to underestimate hyperopia and overestimate myopia [21]. Choong et al. applying a similar cycloplegic protocol to the one in this study, reported a + 0.55 D bias with a table-top autorefractor employing optical infinity simulation fixation and a fogging system, akin to the Myopia Master [1]. Comparisons of Myopia Master autorefraction under cycloplegia with a table-top autorefractor (Nidek ARk-1) and subjective refraction revealed an average more negative SE of -0.43 D and − 0.49D respectively [4]. In contrast, to wavefront-based autorefraction, the Myopia Master exhibited a slightly more negative SE (-0.19 D), compared the Huvitz HRK8000-A and a similar SE (0.05 D) compared to the DNEye Scanner 2 [5, 6].
The bias between cycloplegic and non-cycloplegic autorefraction varies with the type of refractive error, with myopes showing the smallest difference (0.38 D), followed by emmetropes (0.56 D) and hyperopes (1.57 D). This pattern of differences aligns with findings from Fotedar et al. and Hu et al. observed in pediatric populations [22, 23]. These variations impact the Myopia Master’s sensitivity and specificity in classifying refractive errors, with potential false-negative results for hyperopes and false-positive results for myopes, affecting the detection of hyperopes and overestimate the prevalence of myopia in a population [24].
The repeatability of the pre-cycloplegia J0_Ar vector component was lower in hyperopic patients, possibly due to the greater accommodative variability and the influence of accommodation on the J0 refractive component [25]. Additionally, a subtle shift (< 0.125 D) towards with-the-rule (WTR) astigmatism was observed after cycloplegia [26, 27], driven by a decrease in the percentage of eyes with against-the-rule (ATR) astigmatism and an increase in eyes with WTR astigmatism post-cycloplegia.
Keratometry
Cycloplegia demonstrated negligible impact on mean keratometry repeatability, with differences of 0.24 D and 0.27 D observed in pre- and post-cycloplegia measurements, respectively. These values approached the clinical significance threshold of 0.25 D. Similar trends were noted for astigmatic vectors J0_K and J45_K. Garcia-Ardoy et al. conducted a comparative study between Myopia Master keratometry and the IOL Master 700, revealing repeatability limits (0.23 D) consistent with this study, along with comparable astigmatic vector repeatability. Compared to the IOL Master 700 with a repeatability of 0.17 D, the Myopia Master keratometry exhibited slightly reduced repeatability [7].
The examination of keratometry parameters pre- and post-cycloplegia demonstrated no clinically significant differences, with agreement limits closely resembling repeatability limits. This suggests that variability in keratometric measurements pre- and post-cycloplegia aligns with that observed during repeated measurements. Regarding changes in central keratometry post-cycloplegia, these findings align with prior studies reporting no significant differences [11] or minimal clinical relevance (mean change of -0.032 ± 0.121 D) [28]. Other studies noticed corneal flattening post-cycloplegia, ranging from 0.1D [29] to 0.23 D [30]. These variations were attributed to ciliary muscle relaxation during cycloplegia, reducing tension on the scleral spur and resulting in peripheral corneal curvature flattening, exerting only a minor influence on central keratometry [29].
Axial length
Cycloplegia marginally improved AL measurement repeatability (∼1.5x), narrowing the limits from ± 0.14 mm to ± 0.09 mm. This repeatability is comparable to that reported for the Myopia Master in a group of myopic individuals (TRT: 0.11 mm) [7]. Sheng et al. using partial coherence interferometry (IOLMaster), the same biometric principle used by the Myopia Master, reported enhanced post-cycloplegia AL repeatability (TRT: 0.07 mm) compared to pre-cycloplegia (TRT: 0.09 mm) [31]. This improvement may be attributed to the ciliary muscle’s paralyzing effect which reduces crystalline lens thickness fluctuations, enabling a more stable axial length calculation [12].
Although no association between SE differences and AL differences was observed in the present data, a minor elongation of 0.01 mm with LoA near 0.1 mm was noted with cycloplegia. These findings align with previously reported differences ranging from 0.0 to 0.013 mm [11, 28, 31]. Cheng & Hsieh proposed that the observed 0.013 mm elongation observed in their study was associated with a posterior movement of the lens body, compressing the vitreous humour and, subsequently, elongating the AL [28].
Assuming a 0.1 mm variation in AL corresponds to a dioptric change of 0.25D, the repeatability of axial length measurement under cycloplegia enables refractive monitoring below the clinical threshold of 0.25 D. Moreover, since AL repeatability is independent of the AL magnitude, unlike SE measurements, AL measurement may be the most reliable method for monitoring refractive error progression, particularly if performed under cicloplegia.





留言 (0)