
記住我


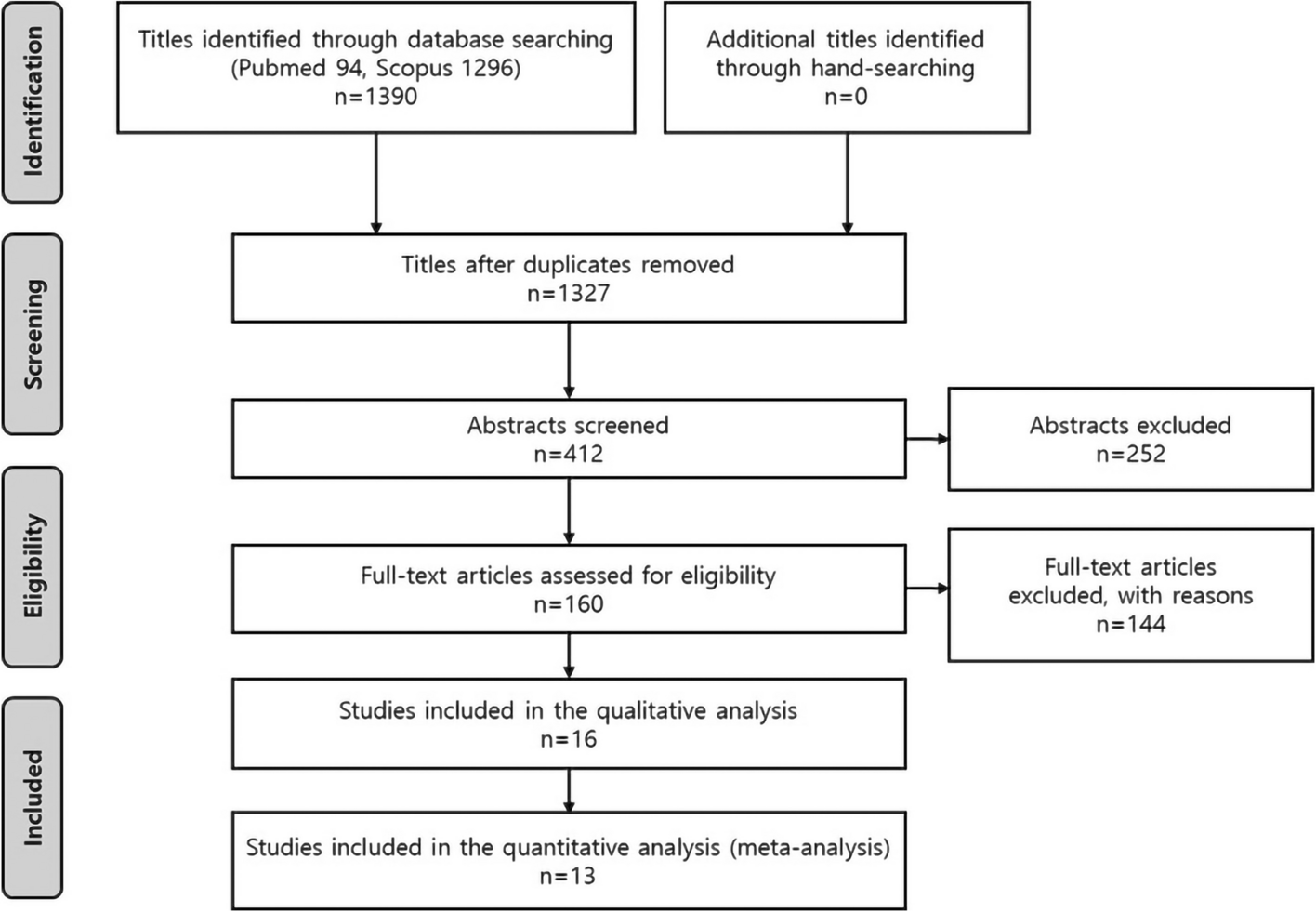



After eliminating duplicate entries, 1747 articles were identified through the search approach. A thorough assessment of titles and abstracts led to the exclusion of articles, leaving 84 articles with potential relevance.
The 84 full-text articles from databases underwent a screening process based on predeterminated inclusion and exclusion parameters. Upon examining the reference lists of these articles, 29 more studies were added. In the end, seventeen studies met the criteria and were incorporated into the review, while 38 were dismissed after a full-text evaluation.
A flowchart depicting the process of identifying, including, and excluding studies along with the reasons for exclusion is presented in Fig. 1.
Fig. 1
Flow chart of the article selection process
Study characteristicsThe systematic review encompassed seventeen studies, with four being cross-sectional [22, 34,35,36], one case report [33], one prospective cohort [41], and eleven randomized controlled trials [11, 16, 23, 24, 26,27,28,29,30,31,32, 40] (Fig. 2). These studies took place between 2013 and 2023, with patients involved in ten studies [22, 23, 25, 27, 28, 31,32,33, 35, 36], animals involved in one study [36], and dental study models involved in five studies [16, 26, 27, 30, 36]. Surgical planning was evaluated in six studies which focused on preoperative maxillary repositioning, occlusion determination, osteotomy plan, cutting, and drilling [16, 22, 25, 27, 30, 36]. The effectiveness of MR technology as an intraoperative navigator was evaluated in six studies [11, 23, 26, 31,32,33]. The intervention was performed using real-time 3D visualization for maxillary reposition, Le Fort I osteotomy, intermediate splint, bimaxillary osteotomy, and mandibular osteotomy.
Fig. 2
Intervention characteristics for duration and accuracy outcome. Left: studies distribution based on intervention. Right: studies distribution based on outcome
The remaining five studies demonstrated the effectiveness of MR technology as a training tool for students, trainees, and oromaxillofacial surgeons to escalate their understanding regarding OGS [6, 7]. The intervention performed on the simulator included face analysis, cephalometry analysis drilling, cutting, oscillating saw usage, osteotomy Le Fort I, mandibular osteotomy, and case-based training. These studies showed the improvement of technical skills and performance between novices and experienced surgeons, as well as the reduction in duration/TCT of OGS procedure.
Among the included studies, the most commonly used software was Dolphin [25], Mimics [33], ManMos [11], VR-Med [33], and Unity 3D engine [26, 33]. The summary of the duration/TCT analysis is presented in Table 3, and the summary of accuracy is presented in Table 4.
Risk of biasUpon evaluating the seventeen studies using the JBI assessment tool, the risk of bias was found to be diverse, with final assessment scores ranging from 68% (moderate risk) [22, 34,35,36] to 100% (low risk) [11, 16, 23,24,25,26,27,28,29,30,31,32,33]. The study exhibits a mix of methodological which should be assessed based on the study designs for interpreting the results.
Out of seventeen studies, five studies included the control group [24,25,26,27,28], facilitating more robust comparisons and outcome evaluations. In contrast, the remaining twelve studies without control groups had limited generalizability and introduced bias into their results [11, 16, 22, 23, 29,30,31,32,33,34,35,36]. The risk of bias assessment of all the studies can be found in Table 5.
Summary of resultsIn the studies reviewed, various assessments were conducted to evaluate the benefits of MR technology in OGS procedure as planning, intraoperative navigation, and pre-surgical training tools by assessing the accuracy, duration/TCT, cost-effective, and knowledge improvements.
Out of the seventeen studies that met the criteria, five studies described the advantages of MR technology about accuracy and TCT/duration [22, 23, 26, 28, 40], three studies explained the advantages about TCT/duration only [16, 25, 27] and six studies described the advantages of MR technology in terms of accuracy only [11, 29,30,31,32,33], while the remaining studies explained the advantages of MR in cost-effective and knowledge improvement [34,35,36].
Accuracy analysis resultThe accuracy defines how close a measurement is to the actual value by comparing the position error (PE), linear/distance error (L/DE), angular error (AE), cutting error (CE), translation error (TE), and orientation error (OE), the accuracy may be evaluated [42]. Gao et al. [26] reported that the position error of the cutting plan and osteotomy by the surgeon was 1.38–4.43 mm, while the engineer position error hits 1.36–3.22 mm. The orientation error was reported similarly between surgeon and engineer (0.88–3.18 mm). In line with that, Ahn et al. [31] indicated a low position error of maxilla reposition, with a mean error of 0.0596 mm.
Distance error was evaluated by several studies to promote the accuracy of MR technology. Koyachi et al. [32] described X-axis as the middle point that passes between the orbitales on both sides, the Y-axis as the vertical cranial direction from the Frankfort horizontal plane, and the Z-axis as the right-hand direction from the center. Zinser et al. [22] observed remarkable accuracy of bimaxillary osteotomy on 16 malocclusion skeletal class III patients with distance error between maxillary landmark to mandibular plane (0.01–0.2 mm), maxillary landmark to coronal plane (0.19–0.37 mm), and vertical dimension to Frankfurt horizontal plane (FHP) to frontozygomatic line (0.12–0.37 mm) with the acceptable angular error between occlusal plane and FHP (< 0.35°).
Ricciardi et al. [29] reveal that MR technology utilization for reconstruction planning and drilling guidance has low distance error and varies between 1.37 and 1.43 mm. Studies by Koyachi et al. [32] and Jo et al. [33] also found low distance error on osteotomy Le Fort I and maxillary reposition, with XYZ deviation 0.38 mm, accuracy of more than 90%, and 2–3 mm distance error. Similarly, Fushima et al. [11] found distance error of mandibular osteotomy approximately < 0.32 mm.
In XYZ direction, Badialli et al. [23] show low distance error on virtual planned osteotomy and maxilla-mandible reposition, with deviation on frontal (1.91 mm), caudal-cranial (0.59 mm), and lateral (1.02 mm). Similarly, Wu et al. [30] found distance error in X direction (0.022–0.648 mm), Y direction (0.047–0.371 mm), and Z direction (0.019–1.139 mm).
Medellin et al. [28] evaluated cutting error after virtual training with and without haptic for mentoplasty and sagittal osteotomy. The use of virtual training only shows cutting error of mentoplasty within 14.6% and sagittal osteotomy within 21.2%. This value was significantly reduced with the combination of haptic-enabled device. The cutting error was reduced to 6.4% for mentoplasty and 4.9% for sagittal osteotomy.
Translation error is defined as the Euclidean distance between the centers of source and target [42]. Lutz et al. [24] utilized VR-Med software and electromagnetic (EM) tracking system for maxilla reposition with translation error within 1.11 mm.
In response to this research, MR technology has proven to be a valuable asset in orthognathic surgery practice, with excellent precision and accuracy. Through seamlessly merging virtual aspects with the actual world, it improves spatial awareness and offers surgeons with comprehensive anatomical visualization. This exact integration improves preoperative planning and provides surgeons with real-time data throughout treatments, providing more predictable and successful outcomes for patients undergoing orthognathic surgery.
Duration/TCT analysis resultTCT is described as the reducement of time or duration needed for surgeons to complete the OGS procedure with the utilization of MR technology [28]. Face analysis and cephalometric analysis are considered important steps in OGS planning. Zaragoza et al. [
留言 (0)