
記住我


Cancer is a lethal disease. Despite continuous work to develop new drugs for cancer, there are still problems facing its treatment. Cancer occurs by tumor cell proliferation with interacting stromal component resulting in a compound tumor microenvironment (TME) [1]. Cancer is not just proliferating malignant neoplastic cells. It is an intricate mass of neoplastic cells along with stromal cells undergoing phenotypic changes that form tumor-associated stroma and actively participate in carcinogenesis [2]. Genomic alterations and inflammatory response by immune cells in the tumor stroma result in certain features characterizing cancer known as hallmarks of cancer. They are sustaining proliferation signals, evasion of growth inhibitory signals, evasion of apoptosis, replicative immortality, prompting angiogenesis, triggering invasion and metastasis, reprogramming of energy metabolism, and evasion of immune destruction [3]. Recently, new enabling characteristics and emerging hallmarks were added: unlocking phenotypic plasticity, non-mutational epigenetic reprogramming, polymorphic microbiomes, and senescent cells [4].
Cancer is a complex genetic disease that is not caused by mutation in just one gene. For instance, one molecular signaling pathway controlling cell growth is disturbed by many genetic aberrations [5]. Since the evolution of genomics, transcriptomics, proteomics, and metabolomics in the current century, the field of targeted therapy has developed. The production of drugs directed toward molecules driving carcinogenesis while minimizing off-target effects is the key of targeted therapy. Cancer targets include growth factors, growth factor receptors, signal transducing molecules, transcription factors, proapoptotic and antiapoptotic proteins [6]. These targets are abnormally expressed in cancer due to genetic mutations of oncogenes and tumor suppressor genes [7]. Genetic mutations can be corrected by using therapeutic nucleic acids (TNAs). The administration of genetic material into living cells to replace a defective gene, promote or repress gene expression to treat a disease is known as gene therapy [8].
MicroRNAs (miRNAs) are non-coding RNAs (ncRNAs) that regulate gene expression by acting on messenger RNA (mRNA). A miRNA binds the 3′ untranslated region (UTR) of a target mRNA to cause gene silencing. miRNAs control many cellular processes such as cell proliferation, differentiation, cell death, and metabolism [9]. The control starts from biogenesis of miRNAs where there are genes in the genome specialized for miRNAs, which are transcribed into primary miRNAs (pri-miRNAs) with stem loops. Pri-miRNA is cleaved by ribonuclease Drosha and its partner DGCR8 to give a shorter stem-loop structure: precursor miRNA (pre-miRNA), which is transported to the cytoplasm for maturation and performing action. The expression of miRNAs is altered in cancer which in turn disturbs the expression of oncogenes and tumor suppressor genes: the main genes driving cancer. miRNAs can be targeted in gene therapy to restore their normal levels [1].
In this review, we will summarize the principle of gene therapy and highlight the RNA interference (RNAi) natural process and method of applying cancer gene therapy. Then, we will elaborate the rising roles of miRNA in diagnosis and treatment of cancer and how to tackle the limitations of its application in treatment.
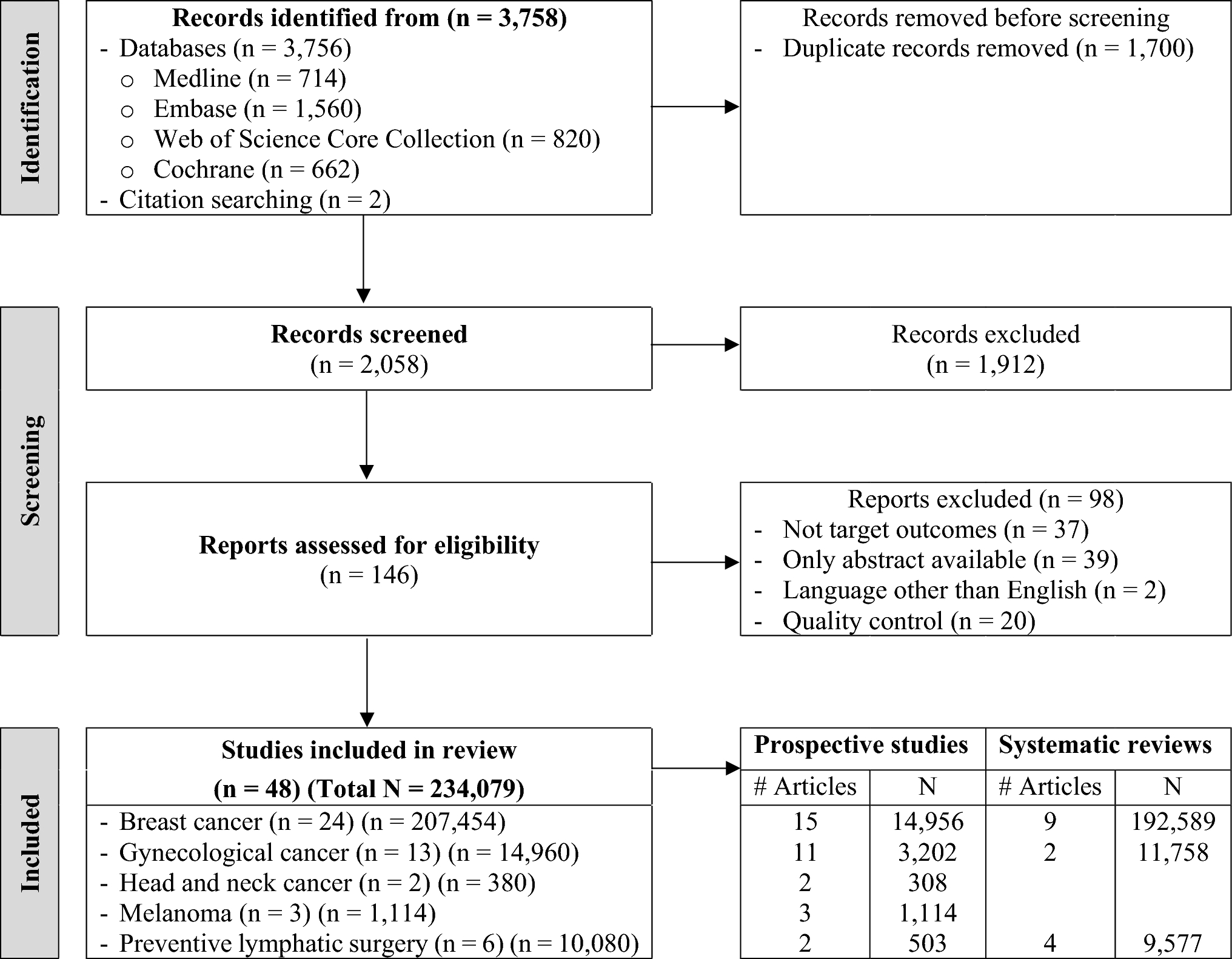
Review search methodologyOnline search on (PubMed, Google Scholar, ScienceDirect) databases was done to identify original research and review articles using the keywords and search terms: “Cancer”, “Targeted therapy”, “Gene therapy”, “Gene expression”, “epigenetic”, “gene therapy vectors”, “nanoparticles”, “antisense oligonucleotides”, “RNA interference”, “microRNAs”, “miRNA”, and “exosomes”. The search was conducted starting from March 2023 to December 2023 considering only English written articles.
Targeted gene therapyThe aim of novel cancer therapies is to provide recovery of patient with increased survival rate and reduced recurrence rate along with preserving the surrounding healthy tissue minimizing as much as possible adverse side effects [10].
Targeted therapy is a mode of cancer therapy depending on administering drugs that target molecules uniquely or differentially expressed in cancer cells in comparison with normal cells. This targeting interferes with tumor cell growth and proliferation. The advantage is that it does not affect normal cells and thus avoiding toxic side effects. Targets can be growth factors, growth factor receptors, signaling molecules, and apoptotic molecules altered by genetic mutations or epigenetic dysregulation [5].
Most agents used for targeted therapy are biopharmaceuticals, which are drugs derived from biological sources. They are made of sugars, proteins, nucleic acids, or may be living cells like reproductive cells and stem cells [11].
Targeting genes can be done by administering nucleic acids into the cell to treat a disease through restoring the function of a mutated gene, regulating gene expression, or synthesizing a new protein. This is the concept of gene therapy. The introduced genetic material may be a gene, segment of a gene, or oligonucleotide and is referred to as transgene [12].
Gene therapy can be used in the treatment of various diseases ranging from inherited to acquired diseases. Many clinical trials have been applied on different diseases with promising results especially single gene disorders [8]. This encouraged researchers to exploit gene therapy for cancer treatment [12].
Gene therapy can be applied in cancer through targeting its molecular processes [1]. Target cells can be cancer cells, normal cells, or immune cells. For cancer cells, the transgene can kill them or regain normal function. While for normal cells, the transgene can shield them from toxicities of a chemotherapeutic drug. Immune cells can also be targeted to recognize and kill cancer cells. The transfer of the nucleic acids is carried out by one of two methods: ex vivo and in vivo. In the ex vivo method, the tumor cells are collected, grown in culture under controlled conditions, manipulated genetically, and inserted back into the host. The in vivo method is applied by introducing the transgene systemically or locally into the tumor cells [12].
There are different modalities for implementing cancer gene therapy such as replacement of tumor suppressor genes, transcription factor decoys, suicide genes, oncolytic viruses, gene editing, oncogene silencing, and targeting miRNAs. Other modalities focus on the TME including immunization gene therapy, targeting angiogenic molecules, cancer-associated fibroblasts, and tumor cell-derived exosomes [1]. The modality nominated for each patient depends on his/her genetic profiling, immune status, and nature of the tumor [12].
RNA-based treatmentThe flow of genetic information from DNA to RNA and from RNA to protein represents the central dogma of molecular biology. The RNA molecule transcribed from DNA and encoding a protein is called mRNA. Cell functions are performed by proteins. RNA molecules that do not give rise to proteins are called ncRNAs but they are involved, by different ways, in regulating gene expression, protein synthesis, and activity. They include ribosomal RNA, transfer RNA, long non-coding RNA, small interfering RNA (siRNA), miRNA, and others. Blocking the step of protein synthesis is the basis of RNAi [13].
Treatment-wise, targeting RNA offers many treatment options and techniques due to the different types of RNAs [13]. Also, acting on the level of RNA is safer than DNA to minimize the risk of mutation. Since RNA is unstable, its delivery into cells is more challenging than DNA where it is subjected to clearance by the kidneys and degradation by endogenous ribonucleases [14]. Chemical modifications are done to the synthetic RNA-based molecules to tackle these obstacles [13] and will be discussed later in this review.
RNA-based treatment can be achieved either through double-stranded (ds) RNA molecule or single-stranded (ss) antisense oligonucleotide (ASO). The dsRNA is converted by ribonucleases into ssRNA that is complementary to the target mRNA and degrade it. The ASO has several mechanisms of action depending on the binding to a specific sequence of the target mRNA: activating RNase H for degradation of mRNA, preventing 5′ cap formation, blocking protein translation, and altering splicing [13].
RNA interferenceRNAi is a physiological process used by the body innate immune system to fight viral infections and as a mechanism of regulating gene expression. mRNA function of coding proteins can be blocked through its degradation or inhibiting the translation process. The result is known as gene silencing. A group of ncRNAs act on mRNAs, the most common are siRNAs and miRNAs [13].
ncRNAs are among the epigenetic factors that control gene expression. Epigenetic modification is any event that affects gene expression without changing DNA sequence. DNA methylation, histone modifications, and ncRNAs are mechanisms of epigenetic modification. Interestingly, there is an interplay between different epigenetic mechanisms. ncRNAs can act on mRNAs that code for enzymes that perform DNA methylation and histone modification: DNA methyl transferase (DNMT) and histone acetyl transferase (HAT)/histone deacetylase (HDAC), respectively. These enzymes also act on promotors of DNA that is transcribed to ncRNAs [15].
One method of applying gene therapy for cancer is oncogene silencing which is based on the process of RNAi. This can be done by introducing a synthetic siRNA or short hairpin RNA (shRNA) that acts on the mRNA of an oncogene such as MYC or KRAS [1].
MicroRNAsmiRNAs are short non-coding ss RNAs [16]. Their length is about 18–25 nucleotides. miRNAs function in regulation of gene expression after transcription by complementary binding to mRNAs [17]. Regulation of the target mRNA is done by one or more of the following processes: translation inhibition, deadenylation, decapping, and mRNA degradation by exonucleases [18]. Several biological processes are controlled by miRNAs such as cell division, differentiation, cell death, and metabolism [19].
The first discovered miRNA was miRNA lin-4. The lin-4 gene was detected in the nematode Caenorhabditis elegans (C.elegans). To the surprise, it did not code for a protein but rather two small RNA molecules ranging from 20 to 70 nucleotides. The longer was the precursor of the shorter. They have sequences complementary to a sequence at the 3′ UTR of lin-14 mRNA [20]. Moreover, mutations in lin-14 result in a phenotype contrasting that of lin-4 mutations and are completely dependent on them [21]. Later, miRNA let-7 was also discovered in C. elegans, and then additionally in multicellular organisms and animals [22]. At present, there are nearly 3000 identified miRNAs in human genomes regulating more than 30% of genes [18].
miRNAs are encoded from different regions in the genome. Intergenic regions are the commonest, followed by introns, exons, long non-coding regions, and repeat regions [18]. These regions are called cancer-associated genomic regions because they are liable to alterations in different cancers [23].
Generation of miRNA starts by transcription from a specific sequence of DNA using RNA polymerase II to produce a pri-miRNA. pri-miRNA is a dsRNA with a stem loop and is cleaved by ribonuclease Drosha and its partner DGCR8 to give a pre-miRNA. pre-miRNA is transported to the cytoplasm through exportin-5 bound to Ran-GTP, where the stem loop is cut by ribonuclease Dicer/TRBP to give a miRNA duplex [24, 25] (Fig.1). The miRNA duplex is loaded into a multicomplex protein called RNA-induced silencing complex (RISC) with Argonaute 2 (AGO2) endonuclease protein as the active part. miRNA is separated into two strands: the guide stand (antisense strand) and the passenger strand (sense strand). The passenger strand is degraded while the guide strand within the RISC complex is directed to the target mRNA. Unlike siRNA, miRNA does not perfectly bind mRNA [26] (Fig.2). There is a specific sequence in the miRNA about 7 bases near the 5′-end that binds to a complementary sequence of the target mRNA at the 3′ UTR or less commonly 5′ UTR or coding region. It is called miRNA seed. Not all other miRNA bases match the mRNA bases [13]. Therefore, a single miRNA can target many mRNAs and an individual mRNA can be targeted by various miRNAs [27].
Fig. 1
MicroRNA processing (Created with BioRender.com)
Fig. 2
MicroRNA mechanism of action. Loading of double-stranded RNA into RNA-induced silencing complex (RISC) with separation of passenger strand that will be degraded. The guide strand along with Argonaute 2 protein and other proteins form active RISC complex that is directed to the target mRNA and acts on it. (Created with Microsoft PowerPoint)
Apart from their standard role in regulation of gene expression through targeting mature mRNA, miRNAs have other targets. Examples are transcripts of introns and intergenic regions, other ncRNAs, circular RNAs, pseudogenes, and short interspersed nuclear elements [18]. This explains the indirect role of miRNAs in regulation of gene expression. Not all mature miRNAs function in the cytoplasm, some are transported back to the nucleus where they carry out other functions such as regulating the maturation of other miRNAs and regulating the expression and maturation of ncRNAs. Also, post-transcriptional regulation of pre-mRNAs in the nucleus can sometimes be done by miRNAs. Moreover, they can act on certain gene promoters causing transcriptional silencing via RNA-induced transcriptional silencing (RITS) complex [28]. Apart from nuclear and cytoplasmic miRNAs, some miRNAs are expressed in extracellular vesicles (ECVs), where they act on other cells [29]. Others are expressed in mitochondria and are involved in mitochondrial functions [30].
It was found that miRNAs regulate the functions of tumor suppressor genes and oncogenes. A miRNA acting on the mRNA of a tumor suppressor gene is classified as oncomiRNA since it inhibits its protective role against cancer. Likewise, a miRNA acting on the mRNA of an oncogene is classified as tumor suppressor miRNA [31]. Studies have found that miRNAs are involved in cellular processes that are disturbed in cancer such as cell proliferation, cell death, migration, and angiogenesis [32]. Oncogenesis does not only arise from genetic mutations and epigenetic alterations in protein-coding genes but also from similar events in miRNAs genes. Furthermore, defects in miRNA synthesis steps share in oncogenesis. For example, loss of function mutation in exportin-5 gene hinders the transport of pre-miRNAs from the nucleus to the cytoplasm and subsequently impairs their processing and functioning [33].
The expression of miRNAs is abnormal in cancerous tissues. miRNA genes are subjected to mutations similar to protein-coding genes such as amplification or deletion. Epigenetic change in the form of methylation of CpG islands of miRNA promoters is also common. In cancer, there is either upregulation or downregulation of miRNAs and it reflects the alterations noted in expression levels of oncogenes and tumor suppressor genes [16]. For example, miRNA-21 is overexpressed in non-small cell lung cancer (NSCLC) and inhibits the activity of PTEN: a tumor suppressor gene [34]. Likewise, miRNA-155 is highly expressed in breast cancer and it downregulates SOCS1 gene [35]. On the other hand, miRNA-29 plays a role in apoptosis and was found to be downregulated in hepatocellular carcinoma. A study conducted by Xiong et al. revealed that the low expression of miRNA-29 was inversely correlated with those of antiapoptotic genes Bcl-2 and Mcl-1 [36]. Another example of tumor suppressor miRNAs are miRNA-34 family members (a, b & c) that are deregulated in various cancers such as leukemia [37], colon cancer [38], prostate cancer [39], head and neck cancer [40], and oral cancer [41].
Some miRNAs can act as oncomiRNAs or tumor suppressor miRNAs in different occasions depending on the target mRNA, since one miRNA has many target mRNAs that can be involved in distinct cellular pathways [16].
Some miRNAs act on enzymes of epigenetic action such as DNMT and HDAC which in turn affect the expression of protein-coding genes. Abnormal expression of miRNAs results in atypical DNA methylation and histone modifications that are associated with oncogenesis. Hypermethylation or hypomethylation of miRNA promotor regions are also causes of aberrant miRNA expression [42]. A study conducted by Kozaki et al. found that miR-34a, miR-137, miR-193a, and miR-203 are downregulated in oral squamous cell carcinoma (OSCC) due to hypermethylated promotor regions [43].
An expression profiling study about OSCC ascertains that upregulated miRNAs are related to tumor suppressor genes, while downregulated miRNAs are related to oncogenes [23]. Decreased expression of miRNA-99A-5p was associated with increased expression of NOX4 in OSCC cells as deduced by Shi et al. [44]. In contrast, Peng and colleagues found that high expression level of miRNA-134 was associated with low expression level of PDCD7 in OSCC tissues [45]. Using bioinformatics tools for mapping functional pathways can reveal the pathways associated with deregulated miRNAs. For example, PI3K/Akt pathway involved in proliferation, migration, and apoptosis is activated in oral cancer and this activation was linked to miRNA-16 and miRNA family let-7, which are downregulated [23]. An experimental study on bladder cancer cell lines concluded the role of tumor suppressor miRNAs-143 and miRNAs-145 on PI3K/Akt signaling pathway [46].
Many miRNAs are involved in the carcinogenesis of cholangiocarcinoma (CCA) by their downstream effects on target genes [47]. For example, miRNA-194 is important in stemness through ECT2 gene [48], while miRNA-329, miRNA-144-5p, and miRNA-451 are important in proliferation and tumor growth through PTTG1 and ST8SIA4 genes, respectively [49, 50]. Moreover, miRNAs such as miRNA-7-5p, miRNA-137, miRNA34a, and miRNA-424-5p play vital roles in CCA progression by triggering invasion, migration, and metastasis. Interestingly, it was found that miRNAs promote CCA by controlling several signaling pathways linked to cancer such as PI3K/AKT, Wnt/β-catenin, NF-κB, p53, Notch, and Hedgehog signaling pathways [47].
Renal cell carcinoma (RCC), the most common cancer of the kidneys, is mediated by dysregulation in miRNAs. miRNAs orchestrate signaling pathways such as RAS/MAPK, Wnt/β-catenin, TGF-β/NF-κB, and VEGF signaling, and dysregulated miRNAs bring about disrupted actions of signaling molecules involved in these signaling pathways which are linked to RCC [51].
Angiogenesis is one of the key features of cancer. In order to survive, cancer cells need blood supply which is preserved through sustained angiogenesis. Like all types of cancer, laryngeal cancer is maintained by angiogenesis and miRNAs have a deep impact on the process [52]. Zhang et al. reported low expression of miRNA-140-5p in laryngeal cancer tissues and transfection of miRNA-140-5p-expressing plasmid in laryngeal cancer cell line inhibited proliferation and angiogenesis. There was negative correlation between miRNA-140-5p expression and VEGF-A expression, which is a main driver of angiogenesis [53].
miRNAs serve as valuable diagnostic and prognostic biomarkers for cancer [32]. Detecting the levels of miRNAs in body fluids can be used for early detection, diagnosis, and monitoring of treatment in different types of cancer [17, 32, 47, 51, 52, 54]. Unlike most RNA molecules in the extracellular environment which are degraded by ribonucleases, extracellular miRNAs detected in body fluids are stable [16]. This could be due to their package in ECVs [29], or loading into high-density lipoproteins [55], or being bound by AGO 2 proteins [56], which protect them from degradation [29]. miRNA profiling denotes detection of their levels in patient’s samples and can be done using laboratory methods including quantitative reverse transcription polymerase chain reaction (qRT-PCR), microarrays, and next-generation sequencing [32]. Ganepola et al. carried out microarray analysis for profiling miRNAs from blood samples that can help in diagnosing early stage of pancreatic cancer [57]. Furthermore, a study conducted by Zhu et al. observed, using qRT-PCR, a number miRNAs with significant higher expression in blood samples of lung cancer patients than healthy controls [58].
miRNAs also act as targets for therapy [23]. Instead of the conventional techniques of gene therapy such as targeting a coding gene or its mRNA, miRNA-based therapy is focused on targeting miRNAs correcting their expression levels. This will subsequently correct the underlying abnormal expression of mRNAs [1].
Treatment using miRNAs can be carried out through two approaches. The first one is based on restoring the function of downregulated tumor suppressor miRNAs by introducing a miRNA mimic. This method is known as miRNA replacement therapy. Transfection of miRNA-340 mimic in NSCLC cell lines reduced cell proliferation and prompted apoptosis as reported by Fernandez et al. [59].
The second treatment approach is inhibiting the function of an upregulated oncomiRNA by a miRNA inhibitor [
留言 (0)