
記住我


The study used secondary national data from the 2017 Korea Community Health Survey performed by the Korea Disease Control and Prevention Agency, collected from August 16 to October 31, 2017. The Korea Community Health Survey is conducted annually with adults aged 19 years or older to examine the health status of residents under the Community Health Act [24]. The survey employed a multistage, stratified, and random sampling method to represent the Korean population.
The primary target population of this study was middle-aged adults living alone. Among the total 228,381 respondents, 10,639 middle-aged individuals (40–64 years of age) from single-person households (5,036 men and 5,603 women) were included in the analysis.
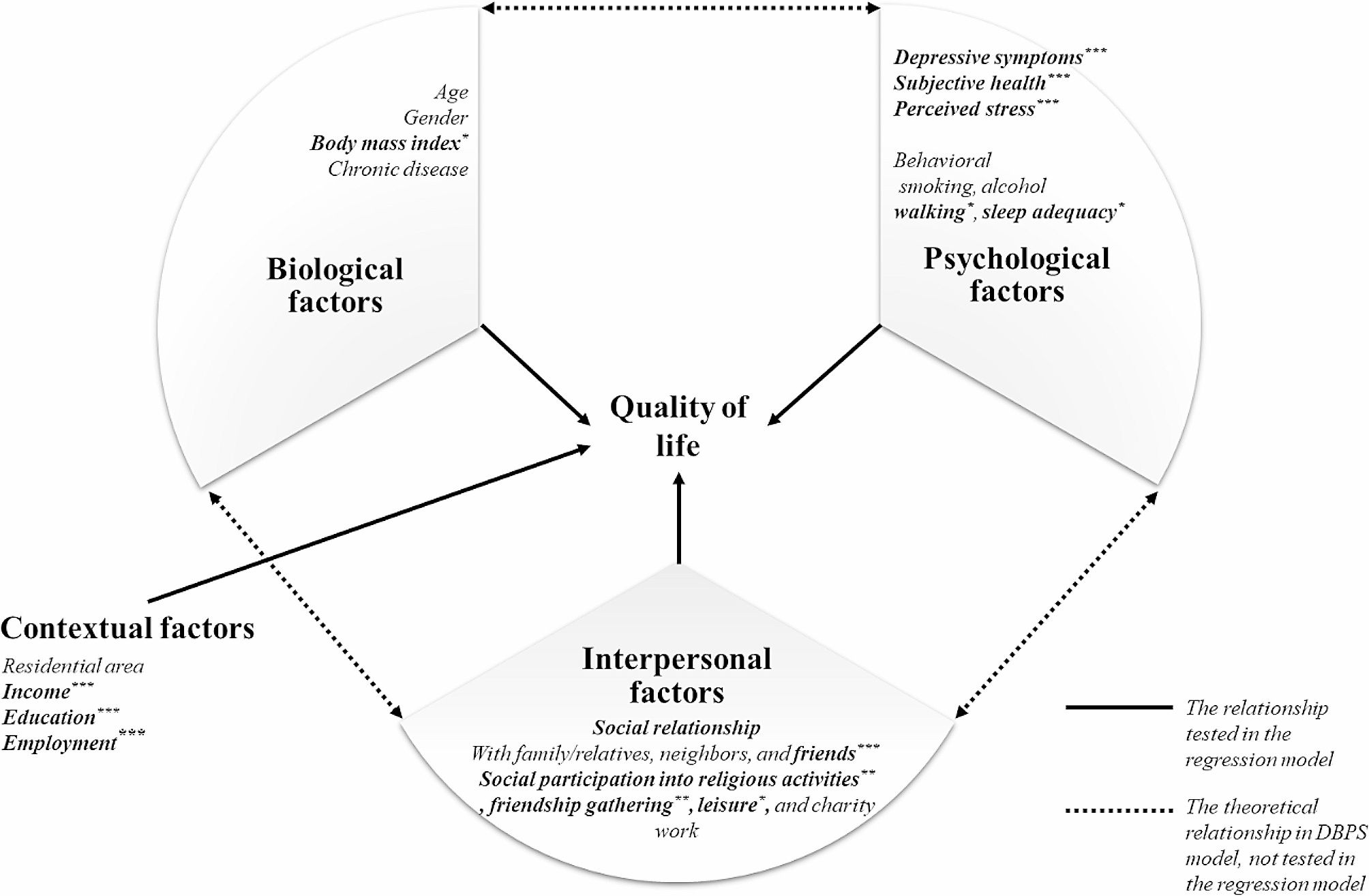
Theoretical frameworkThe DBPS model was developed based on general systems theory and ecological theory by applying ecological perspectives to multidimensional health characteristics [23]. The DBPS model explains health-related factors by dividing them into biological, psychological, and social categories. The social category includes both interpersonal and contextual factors. The factors that influence health are dynamically configured as a set, change continuously over time, and interact with each other. This model offers a multidimensional approach to health and has been applied in various fields [25,26,27]. Figure 1 depicts the conceptual framework of the DBPS determinants of QoL in middle-aged adults living in single-person households.
Fig. 1
Conceptual framework of the dynamic biopsychosocial determinants of quality of life. *p < 0.05, **p < 0.01, ***p < 0.001
Outcome variables: quality of lifeQoL was measured using the EuroQoL-5 Dimension (EQ-5D) [28] to evaluate a standardized basic health index and determine overall health [29, 30]. The EQ-5D measures the following five items: mobility, self-care, usual activity, pain/disability, and anxiety/depression. Each item on current health status was rated on a 3-point scale: 1 point for “no problems,” 2 points for “some problems,” and 3 points for “severe problems.” The total score for responses of “some problems” or “serious problems” was calculated using the weighted QoL formula proposed by the Korea Centers for Disease Control and Prevention: EQ-5D index = 1 − (0.0081 + 0.1140*M2 + 0.6274*M3 + 0.0572*SC2 + 0.2073*SC3 + 0.0615*UA2 + 0.2812*UA3 + 0.0581*PD2 + 0.2353*PD3 + 0.0675*AD2 + 0.2351*AD3). A score closer to 1 indicates a more complete health status [31]. The Korean version of the EQ-5D has been found to be reliable and valid in previous studies [32]. Cronbach’s alpha was 0.757 in this study.
Predictors of quality of lifeBiological factors included age, sex, obesity as determined by height and weight, and the presence or absence of chronic diseases, such as hypertension and diabetes. Obesity was reclassified according to body mass index (BMI), determined by calculating “weight (kg)/height (m2)” based on an individual’s measured height and weight. A BMI of < 23.0 kg/m2 was classified as “normal,” 23–24.9 kg/m2 as “overweight,” and ≥ 25.0 kg/m2 as “obesity” [33].
Psychological factors were measured based on depressive symptoms, subjective health levels, subjective stress levels, and health-related behavioral factors such as current smoking, drinking, exercise, and sleep hours. Depressive symptoms were assessed using the Patient Health Questionnaire-9, with total scores ranging from 0 to 27 points. Depression severity was categorized into two groups: minimal to mild (~ 9 points) and moderate to severe (10 ~ 27 points). Cronbach’s alpha was 0.834 in this study.
Subjective health levels were measured on a 5-point scale ranging from 1 point for “very good” to 5 points for “very bad” in response to the question: “How do you usually think of your health?” This was used to determine respondents’ health status––the higher the score, the higher the subjective health.
Subjective stress levels were measured to assess stress levels in daily life (study, work, and housework) based on responses to the following question: “How much stress do you usually feel in your daily life?” This item was measured on a scale ranging from 1 point for “I feel very stressed” to 4 points for “I hardly feel stressed.” Higher scores indicated higher subjective stress levels.
Current smoking status was measured by asking participants about current (“yes”) versus past (but not current) smoking habits and never smoking at all (“no”). Current drinking status was measured by asking participants whether they engaged in binge drinking. Regular walking was defined as walking at least 5 days per week for at least 20 min per day. Sleep adequacy was defined as 7–8 h of sleep per day.
Interpersonal factors were measured based on respondents’ social networks and participation in social activities. Social networks were assessed to determine the frequency of contact with relatives, family members, neighbors, and friends who were available for direct two-way communication in person or by telephone. The respondents were asked to list the person they contacted most frequently, which was measured as an ordinal variable: less than once a month, once a month, 2–3 times a month, once a week, 2–3 times a week, and more than 4 times a week. For the analysis, this variable was recoded as < once/week, 1–3 times/week, and ≥ 4 times/week.
Social activities included religious activities, friendship gatherings, leisure activities, and charitable work. Respondents were asked to answer “yes” or “no” to the following question: “Do you regularly participate in each category of social activities at least once per month?”
Contextual factors included residence, monthly household income, education level, employment, and marital status. Residential areas were divided into urban and rural. Monthly household income was measured as the average monthly household income over the past year. Based on the 2017 median income of single-person households (KRW 1,652,931), single-person household income was classified into two groups: < KRW 2 million and ≥ KRW 2 million. Education level was reclassified as a high school diploma or higher, and employment status was recorded as currently employed or unemployed. Marital status was recorded as married, divorced, separated, widowed, or never married.
Statistical analysisConsidering the data structure of the multistage stratified cluster sampling method used in the Korea Community Health Survey, a complex samples statistic was used for the analysis. Complex samples descriptives and crosstabs statistics were used to examine the differences in the score of EQ-5D by each variable of DBPS factors. A complex samples general linear model was used to determine the predictors of QoL by biological, psychological, behavioral, interpersonal, and contextual factors. The predicting model was estimated again for the DBPS model, using all potential predictors from the biological, psychological, behavioral, interpersonal, and contextual factors. Unstandardized b coefficients (B) with 95% confidence intervals (95% CI) were estimated. A p-value < 0.05 indicated statistical significance. All statistical analyses were performed using IBM SPSS version 29.0 (New York, NY, USA).
留言 (0)