
記住我


The NHANES is a national cross-sectional study in the United States. It can be accessed through the Centers for Disease Control and Prevention National Center for Health Statistics (NCHS; https://www.cdc.gov/nchs/). The NHANES employs a complex, multistage probability sample design and conducts surveys of 5000 people every two years on average. Data from 2017 to 2020 were combined to perform this cross-sectional analysis. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline [15].
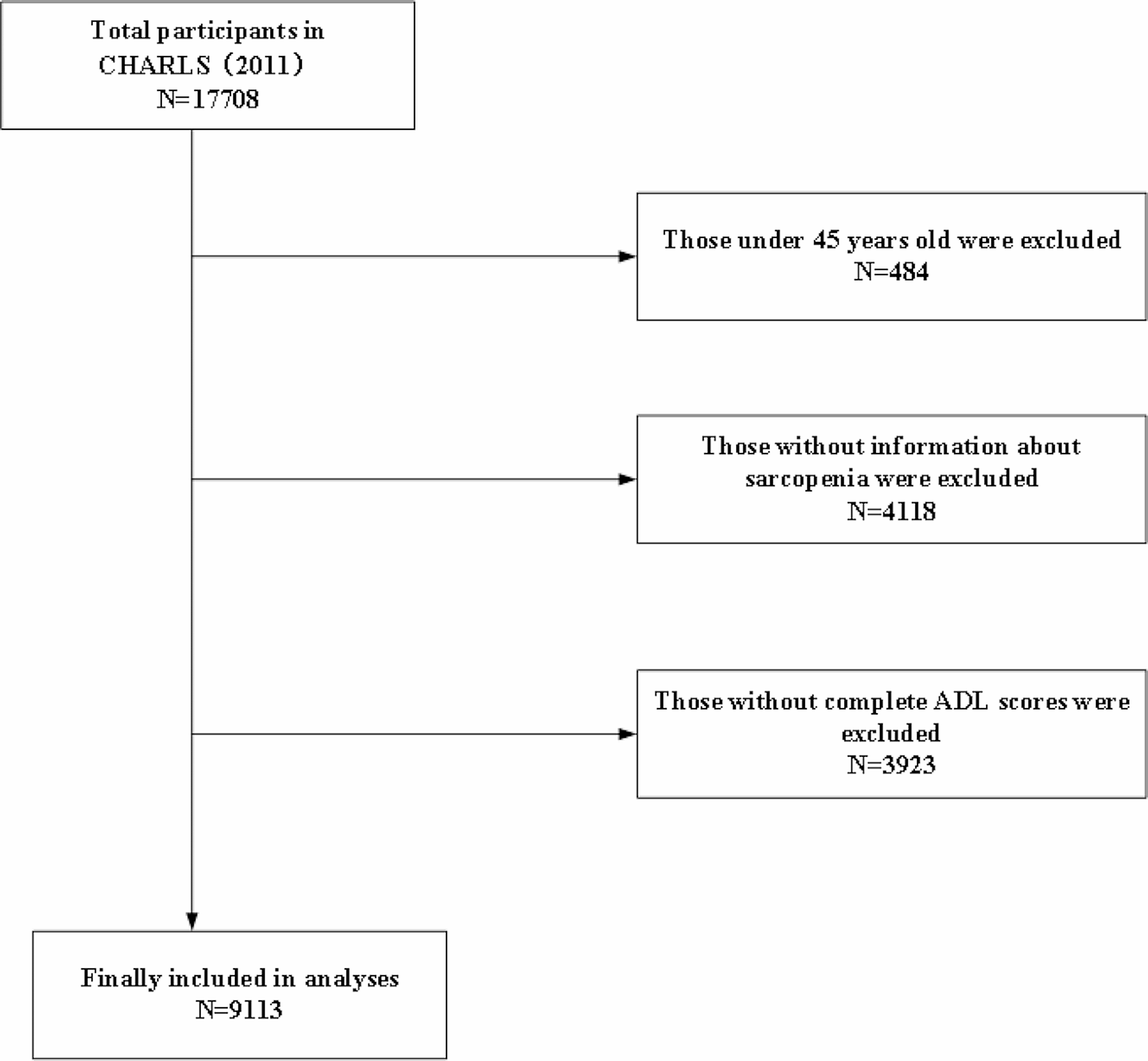
This cross-sectional study included 15,560 participants from the nationally representative consecutive NHANES 2017–2020, individuals were excluded if (1) under 20 years of age; (2) missing data on LE8; (3) missing elastography examination; (4) missing any values for demographic and questionnaire data. Ultimately, a total of 5646 participants were finally enrolled. Figure 1 shows the data processing details.
Fig. 1
Flowchart of study participants
Study covariatesCovariates consisted of demographic characteristics, several factors previously displayed or assumed to be associated with LE8 or MASLD, including gender, age, race, education, marital status, poverty-to-income ratio (PIR), body mass index (BMI), low-density lipoprotein cholesterol (LDL), high-density lipoprotein cholesterol (HDL), plasma triglyceride, waist circumference, fasting serum glucose, glycohemoglobin type A1c (HbA1c), blood pressure, drug treatment, alcohol use, diabetes mellitus, cigarette use.
Definition of MASLDHepatic steatosis in this study was defined by the controlled attenuation parameter (CAP), obtained via vibration controlled transient elastography (VCTE), which is a validated tool for measuring steatosis in participants with fatty liver [16]. CAP ≥ 268 dB/m was defined as significant hepatic steatosis [17]. The diagnosis of MASLD is based on hepatic steatosis and requires the fulfillment of at least one of five: (1) BMI ≥ 25 kg/m2 (≥ 23 kg/m2 in Asian) or waist circumference > 94 cm in men, > 80 cm in women, or ethnicity adjusted; (2) Fasting serum glucose ≥ 100 mg/dL (≥ 5.6 mmol/L) or 2-hour post-load glucose level ≥ 140 mg/dL(≥ 7.8 mmol/L) or HbA1c ≥ 5.7% or on specific drug treatment; (3) Blood pressure ≥ 130/85 mmHg or specific drug treatment; (4) Plasma triglycerides ≥ 150 mg/dL (≥ 1.70 mmol/L) or specific drug treatment; (5) Plasma HDL cholesterol < 40 mg/dL (< 1.0 mmol/L) for men and < 50 mg/dL (< 1.3 mmol/L) for women or specific drug treatment [1].
Measurement of LE8The components of LE8 include 4 health behaviors (diet, physical activity, nicotine exposure, and sleep duration) and 4 health factors (body mass index, non-high-density-lipoprotein cholesterol, blood glucose, and blood pressure). Each metric has a scoring algorithm ranging from 0 to 100 points, allowing generation of a new composite CVH score (the unweighted average of all components) that also varies from 0 to 100 points. Detailed algorithms for calculating the LE8 scores for each of the metrics to NHANES data have been previously published and can be found in Supplementary File 1. The overall CVH scores of 80 to 100 be considered high CVH; 50 to 79, moderate CVH; and 0 to 49 points, low CVH [10].
Dietary indicators were assessed using the Healthy Eating Index (HEI) 2015 measured by the subjects’ 24-h dietary review [18]. Physical activity, nicotine exposure and sleep data were collected through a self-report questionnaire. Details of the questionnaire can be found in Supplemental File 2. The body measures data include height and weight, height was defined as standing height. Those data were collected, in the Mobile Examination Center (MEC), by trained health technicians. The health technician was assisted by a recorder during the body measures examination. BMI was obtained by dividing weight (kilograms) by the square of height (meters). All blood pressure determinations (systolic and diastolic) are taken in the MEC. After resting quietly in a seated position for 5 min and after the participant’s maximum inflation level (MIL) has been determined, three consecutive blood pressure readings are obtained. NHANES collected the fasting blood sample for laboratory analysis, including plasma glucose, HbA1c, HDL, and total cholesterol. Non-HDL cholesterol was obtained by subtracting HDL from total plasma cholesterol.
Statistical analysisDue to the complexity of the NHANES sampling design, appropriate weights were used for the sample analysis. For baseline characterization, weighted means (standard errors) were used for continuous variables, and sample sizes (weighted percentages) were used for categorical variables. Survey-weighted multivariable logistic regressions were used to investigate the independent association of LE8 and different degrees of CVH with the risks of MASLD. Crude models did not adjust for any potential confounders. Model 1 adjusted for age, sex, race. Model 2 was further adjusted for education, marital status. Restricted cubic spline (RCS) was also used to further validate the link between LE8 scores and its subscales score with MASLD. To examine different subpopulations at baseline, subgroup analyses were performed by gender, age strata, race, education levels, marital status and ratio of family income to poverty. For sensitivity analyses, we excluded the individuals with comorbidity (including CVD, COPD, and cancer) to assess the robustness of our findings. Statistical significance was ascertained by a two-sided P value of < 0.05. All statistical analyses were performed using R software, version 4.2.2 (R Core Team, Vienna, Austria).
留言 (0)