Our study aims to analyze the impact of sarcopenia in hospitalized elderly patients. We deliberately conducted the study in a cohort of cirrhotic patients, comparing it with non-liver disease patients to highlight differences. Thus, the elderly cirrhotic population often develops sarcopenia. Therefore, we aimed to verify whether the characteristics of sarcopenia in this population were consistent with those of the general reference population. The explored population exhibited significant comorbidities, including arterial hypertension, type 2 diabetes mellitus, and dyslipidemia. Clinical features included increased BMI and a risk of malnutrition (assessed by MNA). The population was stratified into elderly patients with advanced liver disease and compared with those without such pathology. Cirrhotic patients accounted for 43.47% of the total population. Both cohorts, in terms of anthropometric assessment, muscle strength (analyzed by handgrip), and nutritional evaluation, were homogeneous. Laboratory parameters differed between cirrhotic and non-liver disease patients, with cirrhotic patients showing reduced platelet and white blood cell counts and elevated total and indirect bilirubin, GOT, ALP, and INR. These conditions are attributed to underlying pathology, including portal hypertension-associated splenomegaly and hepatic synthesis deficit. Patients were classified based on the European Working Group on Sarcopenia in Older People. Probable sarcopenia was identified with a prevalence of 62% in cirrhotic patients and 63% in non-cirrhotic patients, with no statistically significant differences observed. As known, the original operational definition of sarcopenia by EWGSOP was a major change at that time, as it added muscle function to former definitions based only on detection of low muscle mass. Revised guidelines, consider muscle strength the forefront, as it is recognized that strength is better than mass in predicting adverse outcomes [23]. Based on the loss of muscle strength, probable sarcopenic patients were further classified into two groups: “confirmed sarcopenia” (those who experienced both muscle mass and strength loss) and “dynapenic” (those who only lost muscle strength). We did not find any significant difference in the prevalence of this condition between cirrhotic and non-cirrhotic patients. However, considering the hypoalbuminemia typically encountered in cirrhosis, we would have expected some significant differences regarding dynapenia. This lack of distinction may be attributed to the small number of individuals in the subpopulation.
To better define whether there is a relationship between muscle mass and malnutrition, we performed a correlation analysis between appendicular muscle mass and the previously listed anthropometric-laboratory parameters. Positive correlations were observed between appendicular mass and height, weight, BMI, arm circumference, calf circumference, handgrip, and MNA, indicating that ASM assessment correlates with anthropometric parameters, malnutrition risk, and grip strength. An inverse correlation was found between ASM and total cholesterol, HDL, LDL, and ESR, suggesting a relationship between muscle mass and lipid profile and inflammation. Literature supports the concept of “lipotoxicity,” a pathologic condition explaining the evolution process in sarcopenia, indicating a vicious cycle between sarcopenia and ectopic fat accumulation through mitochondrial dysfunction, proinflammatory cytokine production, oxidative stress, collagen deposition, extracellular matrix remodeling, and lifestyle habits. The exacerbation of lipotoxicity in sarcopenia may lead to increased disability, morbidity, and mortality [29, 30]. The correlation between ASM and collected parameters was further explored in cirrhotic and non-liver disease patients. Both populations showed positive correlations for height, weight, calf circumference, and handgrip. In non-liver disease patients, ASM also correlated positively with BMI, MNA, and arm circumference but negatively with total cholesterol and LDL, suggesting the influence of malnutrition degree and lipotoxicity on sarcopenia in non-liver disease patients. In contrast, in cirrhotic patients, appendicular mass correlated negatively with GPT values, a liver damage-specific index, indicating that cirrhotic patients with greater liver damage had lower appendicular muscle mass. It's worth noting that cirrhotic patients showed no correlation with the MNA, suggesting that sarcopenia in cirrhosis is not correlated with malnutrition but rather with the alteration of the muscular component. The presence of sarcopenia has been shown to be associated with increased risk of falls and fractures, development of acute decompensation or acute-on-chronic liver failure, and death in patients with cirrhosis [31]. In a recent extensive meta-analysis, Tantai et al. illustrated that sarcopenia affects approximately one-third of patients with cirrhosis, correlating with a roughly twofold higher risk of death among affected patients. This association remained consistent across nearly all patient subgroups, including those with low MELD scores [2].
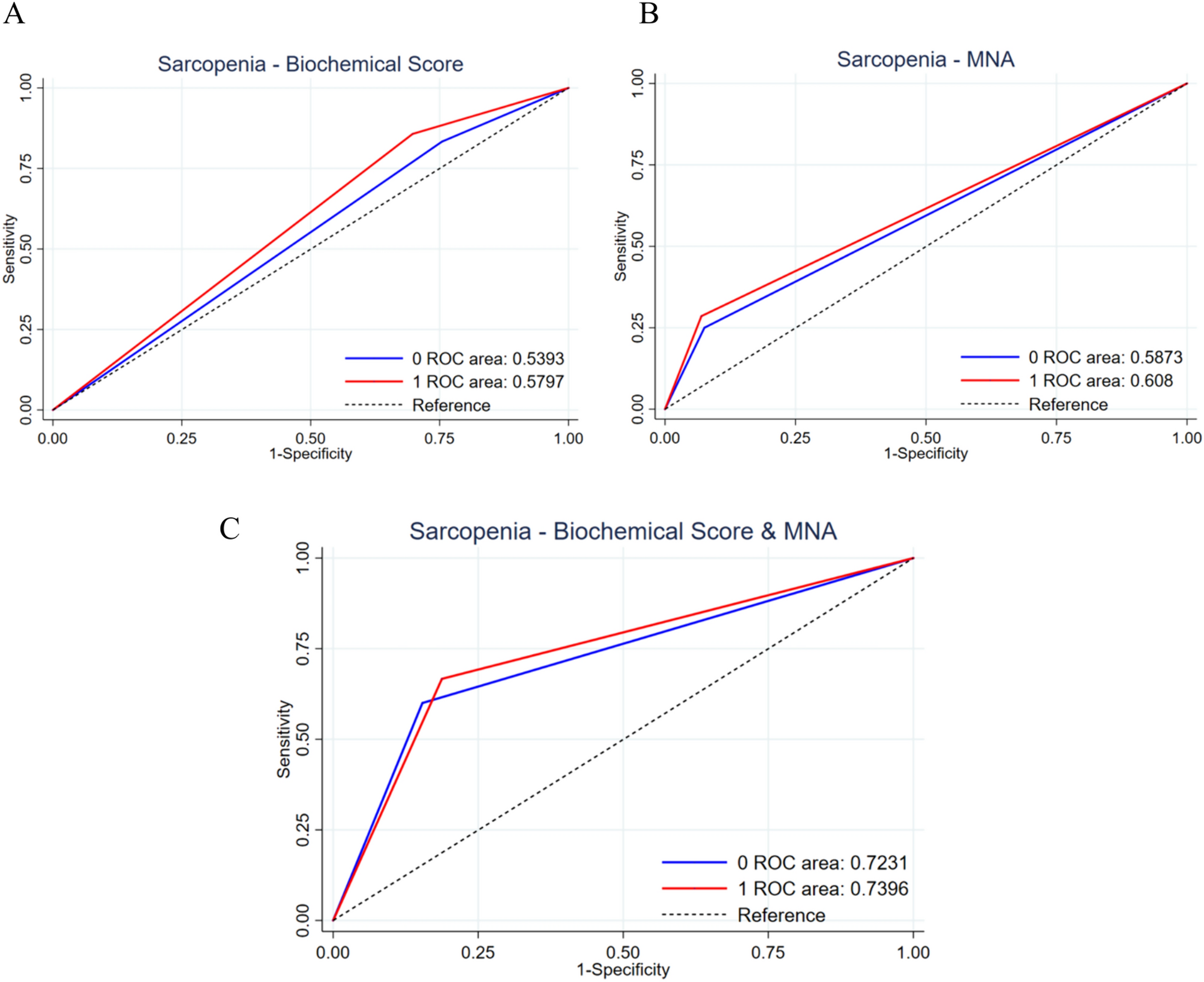
Therefore, we questioned how we could stratify the prognosis of cirrhotic and sarcopenic patients quickly and non-invasively. Analysis of the odds ratio in the elderly hospitalized population for parameters associated with sarcopenia demonstrated a strong capability to assess the likelihood of sarcopenia, especially when utilizing the MNA score in conjunction with the biochemical score. Finally, the analysis of AUROC, evaluating the test's accuracy in predicting sarcopenia, demonstrated good sensitivity when employing the composite score incorporating altered nutritional risk markers and reduced MNA. These results are consistent with literature emphasizing the importance of malnutrition in sarcopenia assessment, associated with about four times higher risk of developing it, sometimes in a severe form [32, 33].
In conclusion, considering the progressive demographic aging, sarcopenia will have a strongly negative prognostic and economic impact on public health. It is associated with an increased risk of short- and long-term mortality, reduced overall survival, an increased risk of serious complications, and prolonged hospitalization [34]. Our study demonstrated that sarcopenia is a pathologic condition present in the hospital setting, both in the general population and in patients with liver cirrhosis, with no significant differences in terms of prevalence. Sarcopenic patients exhibited lower anthropometric and malnutrition screening test values than their non-sarcopenic counterparts. Calculated muscle mass in the cohort of hospitalized elderly patients correlated directly with anthropometric parameters, especially with MNA, and thus with the degree of malnutrition, while being inversely correlated with lipid profile and systemic inflammation. When analyzing the association between ASM in cirrhotic and non-liver disease patients, significant differences emerged, such as the direct correlation in non-cirrhotic patients with the MNA value compared to cirrhotic patients, and the inverse correlation with the lipid profile present in the non-liver disease population compared to cirrhotic patients. Both populations, however, showed a direct correlation with height, weight, calf circumference, and handgrip, emphasizing the link between muscle strength and muscle mass. Finally, in cirrhotic patients, muscle mass was inversely correlated with GPT, indicating the role of chronic liver damage.
The main limitation of the study is the small number of individuals in the subpopulation, particularly when considering the distinction between confirmed sarcopenia and dynapenia. This limitation hinders the ability to draw significant conclusions regarding the expected differences, especially regarding dynapenia, in the context of hypoalbuminemia typically encountered in cirrhosis. In addition, the study acknowledges the potential influence of the small sample size on the observed relationships and correlations, which may limit the generalizability of the findings. To address this limitation, forthcoming studies could focus on enrolling larger cohorts of patients, enabling more thorough analyses and comparisons across subgroups. Furthermore, longitudinal studies could be undertaken to evaluate the progression of sarcopenia over time and its effects on clinical outcomes in elderly patients with liver disease.
Our analyses revealed that assessing nutritional status using MNA and combining it with biochemical markers of nutritional deficiency, such us transferrin, albumin, total cholesterol, lymphocyte count and C-reactive protein is more sensitive and specific for screening sarcopenia in hospitalized elderly patients, even in the absence of significant differences between cirrhotic and non-cirrhotic patients. In our study, we initially recognized the potential value of incorporating validated biochemical scores such as the CONUT score or Prognostic Nutritional Index (PNI) to assess nutritional status and predict adverse outcomes in in-hospital patients across diverse settings [35, 36]. However, upon closer examination, we encountered limitations in the ability of these scores to adequately define the state of sarcopenia in cirrhotic patients, particularly those in end-stage disease. The inclusion of total cholesterol count in the CONUT score and the reliance on lymphocyte count in both the CONUT and PNI scores posed challenges in accurately characterizing sarcopenia in this specific patient population. Consequently, we chose to augment our analysis by integrating nutritional parameters with anthropometric and biochemical indicators such as transferrin and C-reactive protein. This approach allowed for a more comprehensive evaluation of sarcopenia in cirrhotic patients, with particular attention to its impact on muscle mass. Furthermore, we employed the Hwang equation to estimate appendicular muscle mass, enhancing the precision of our assessments.
Collectively, our findings indicate that: (1) sarcopenia should be included in the initial assessment of all patients with cirrhosis; (2) regular monitoring for sarcopenia is warranted in all cirrhosis patients, irrespective of the severity of hepatic dysfunction; (3) further research is essential to integrate sarcopenia or muscle mass index/function into a structured prognostic scale for cirrhosis patients.
Our study achieved its primary endpoint by assessing sarcopenia in elderly hospitalized patients with advanced chronic liver disease and comparing it with non-hepatopathic patients, while examining correlations with anthropometric and biochemical factors. In addition, the secondary endpoint was achieved by identifying a diagnostic test capable of predicting the risk of sarcopenia in the elderly, particularly in cirrhotic patients at high risk of malnutrition. Therefore, a thorough screening and assessment of sarcopenia and nutritional status in hospitalized patients should be carried out. This is crucial for implementing nutritional and multidisciplinary intervention programs, especially in liver-suffering populations at high risk of disease and loss of independence.



留言 (0)