
記住我


Burn injuries are one of the most painful traumas, have long-term physical and psychological impacts, and are extremely difficult to manage. Severe burns require intensive management of both long-term pain due to burns and short-term acute pain due to procedures such as dressing changes [1]. Opioids have been established as a basic pain management therapy in patients with severe burns because of their excellent efficacy in providing adequate analgesia [2,3,4]. Fentanyl, a synthetic opioid, has both efficacy and potency for pain and is known to have a lower risk of side effects than morphine [1, 2]. Therefore, fentanyl is widely used as an analgesic and sedative in patients with severe burn injuries in intensive care units (ICU).
Initial burn shock is a hypodynamic and hypovolemic state, with rapid fluid loss from the intravascular space and decreased cardiac output, which lasts for the first 24–48 h [5, 6]. Therefore, organs in the burn shock stage require large volumes of fluid infusion, which rapidly dilutes plasma proteins and expands the intravascular volume. Moreover, after successful fluid resuscitation after burn shock, a hypermetabolic state occurs with increased cardiac output and reduced systemic vascular resistance [7, 8]. Increased cardiac output during a hypermetabolic state leads to increased hepatic, splanchnic, and renal blood flow, resulting in increased metabolic and renal clearance of drugs [7, 8]. Therefore, patients with severe burns have the potential to influence the pharmacokinetics (PK) of many drugs, including fentanyl, owing to pathophysiological changes and therapeutic interventions (e.g., hemodynamic alterations, organ failure, and capillary leak).
An intravenous bolus of fentanyl in patients with burns has been reported to result in lower blood concentrations than in patients without burns [5, 9, 10]. In contrast, continuous intravenous infusion of fentanyl has recently been recommended for burn pain management [4], but there are few reports on PK alterations in patients with burns treated with continuous intravenous fentanyl infusion. Here, we report the clinical course and changes in blood fentanyl concentrations during the acute phase in a patient with severe burns treated with continuous intravenous infusion of fentanyl.
CaseThe patient was a woman in her 40s with a history of hypertension, hyperthyroidism, and insomnia. The patient was transported to our hospital with burns caused by a gas cylinder explosion. On admission, the level of consciousness was I-1 on the Japan Coma Scale and 15 on the Glasgow Coma Scale. Her vital signs were as follows: blood pressure, 121/84 mm Hg; respiratory rate, 20 breaths/min; pulse rate, 106 beats/min; and SpO2, 99% (O2 was 10 L). The admission weight of patient was 45 kg, and burns had spread to the face, neck, shoulders, and all four extremities, with a total burn area of 39.0% (14% third-degree and 18% second-degree; burn index, 23; prognostic burn index, 76). Based on her consciousness, respiratory status, and bronchoscopic findings, intubation was not performed. Table 1 shows the laboratory values at admission. Organ failure, such as liver or renal dysfunction, was not observed. The patient underwent fluid resuscitation based on the method of Baxter (7644 mL) during the first 24 h, and then the fluid volume was adjusted according to the urine volume. Although accurate assessment of blood pressure was difficult during the burn shock stage owing to pain-related body movements, the patient’s systolic blood pressure (sBP) was maintained in the range of 90–120 mmHg during the burn shock stage on days 1 and 2. From day 3, after the burn shock stage had resolved, the sBP was maintained in the range of 110–140 mmHg. Therefore, during the treatment period, her hemodynamic parameters, including blood pressure and pulse rate, were maintained.
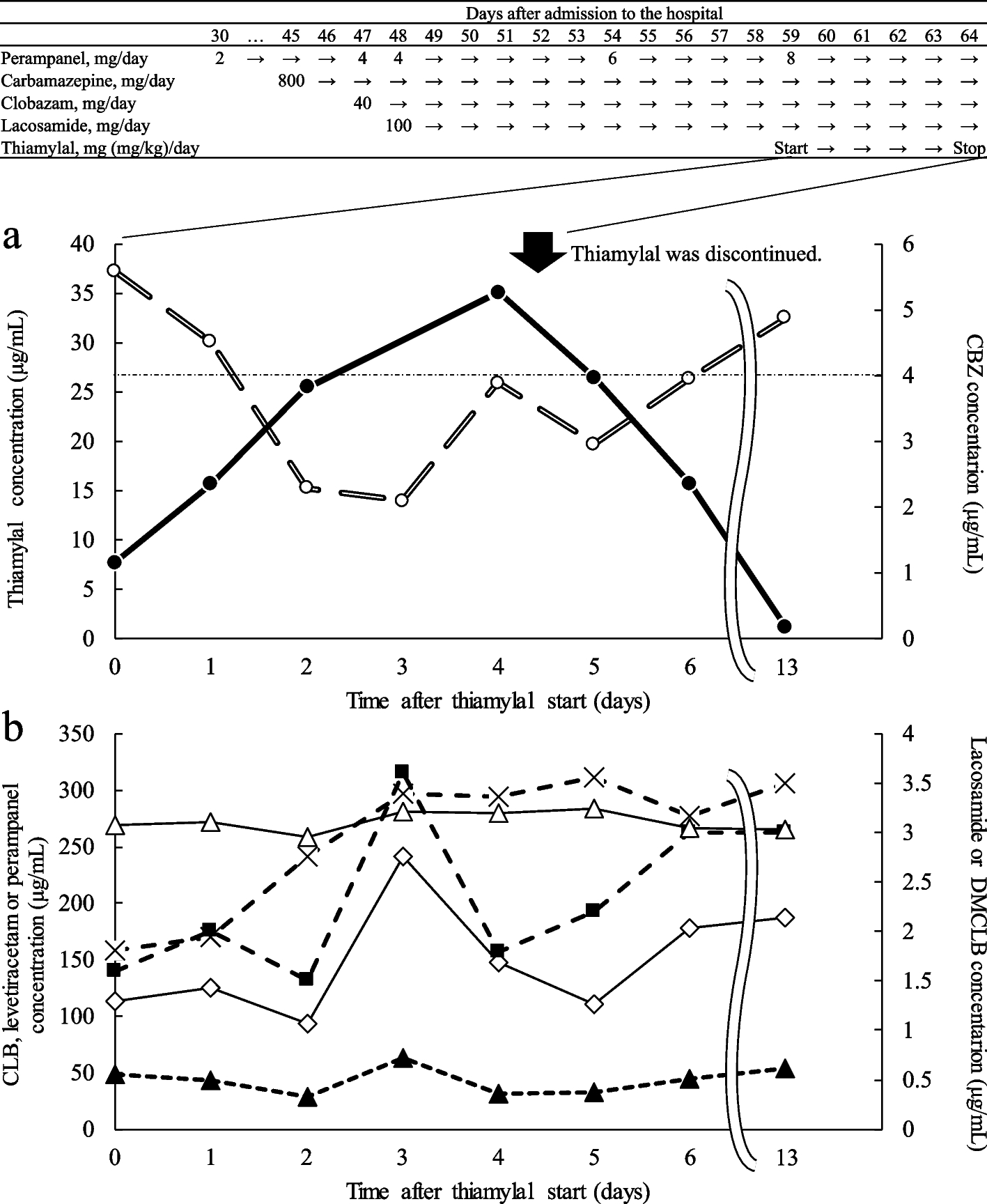
Table 1 Results of the blood test performed on hospital arrivalThe numerical rating scale (NRS) score for pain assessment was 7 points immediately after admission. The patient’s clinical course and pain management since admission are shown in Fig. 1. For pain relief, the patient received a continuous infusion of 0.01 mg/mL fentanyl (100 µg/h) after the fentanyl flush (50 µg). Three hours after starting fentanyl infusion, the rate of continuous infusion of fentanyl was adjusted to 20 µg/h. The rate of infusion was determined by fentanyl dose simulation based on Shefer’s PK parameters [11] to achieve a target blood concentration of 1.0–1.5 ng/mL. On day 1, the NRS score remained between 3 and 6 points, and pain control was inconsistent, even though fentanyl blood levels had reached a steady state. Thus, before day 2, fentanyl administration rate was temporarily increased from 20 µg/h to 30 µg/h. However, the NRS score remained between 3 and 6 points on day 2, and pain management was difficult. After this, the fentanyl administration rate was kept constant at 30 µg/h to avoid the risk of respiratory depression, as the patient was not intubated during the treatment period. The main therapeutic interventions on days 1 and 2 were massive fluid loading, analgesia with fentanyl, administration of a proton pump inhibitor, and debridement; no deep sedation was used during the treatment period.
Fig. 1
Clinical course of the patient
The black points indicate the observed values, and the white points indicate the predicted values. The predicted concentration curves were analyzed using fentanyl dose simulation based on Shefer’s pharmacokinetic parameters. The number in parentheses in the Out item indicates the urine volume (mL/day)
ALT, alanine aminotransferase; AST, aspartate aminotransferase; CFPM, cefepime; div, drip infusion into vein; ER, emergency room; iv, intravenous injection; NRS, numerical rating scale; VCM, vancomycin
On day 3, when the burn shock stage resolved, the NRS was 2 points, and pain control improved. Moreover, fentanyl administration rate was able to be reduced from 30 µg/h to 20 µg/h. From that day onward, the NRS remained 2 points and complaints of pain decreased, without changing the fentanyl administration rate. The main therapeutic interventions from days 3 to 7 were analgesia with fentanyl, administration of proton pump inhibitors and antibiotics, and debridement. Moreover, during the NRS assessment period, the only analgesics used were fentanyl and ketalar, as shown in Fig. 1.
To investigate the cause of difficulty in controlling pain during the acute phase, serum fentanyl concentrations were measured on days 1, 2, 3, and 6 using liquid chromatography-tandem mass spectrometry (LCMS-8045 triple quadrupole mass spectrometer; Shimadzu, Japan). In our measurement methods, no background peaks interfering with the fentanyl peak were observed. Moreover, fentanyl showed good linearity with an R2 value > 0.99 in the range of 0.05–1 ng/ml serum concentration, and the results were reproducible (supplementary Fig. 1). The patient’s serum fentanyl concentrations were as follows: 0.50 ng/mL on day 1, 0.66 ng/mL on day 2, 1.07 ng/mL on day 3, and 0.73 ng/mL on day 6. We found that the fentanyl concentrations on days 1 and 2, when the pain was not controlled, were only approximately 50% of the predicted concentrations. However, after the burn shock phase resolved (after day 3), serum fentanyl concentrations gradually approached the target range, even though the fentanyl administration rate from day 2 to day 3 remained unchanged. And the NRS score improved from day 3.
Written consent for the publication of this case report was obtained from the patient as per the Guidelines for Privacy Protection in Medical Papers and Conference Presentations, including Case Reports (Japan Surgical Society) [12]. This case report was not subjected to formal review by the Ethical Review Board of Fukuoka University Hospital.
留言 (0)