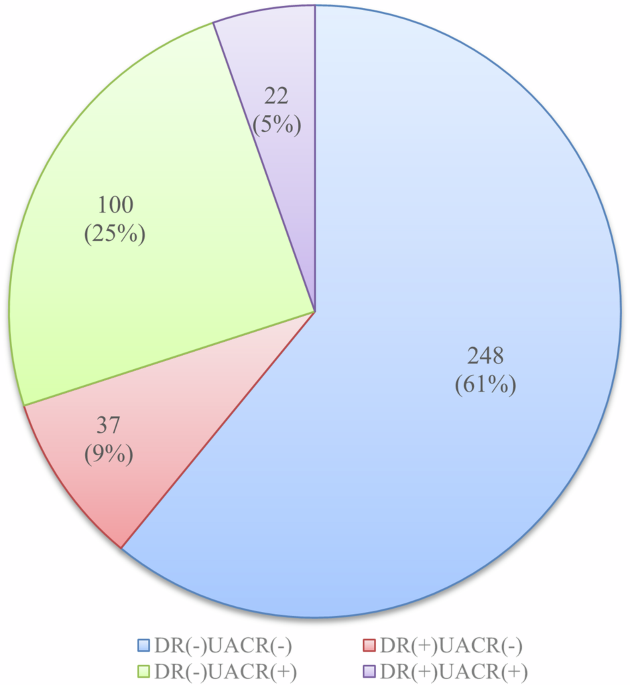
The first finding of our research was the distribution of microvascular complications in diabetes in the outpatient population. Among the enrolled outpatient population, about 61% of the people fall into the group DR(–)UACR(–), 9% fall into the group DR( + )UACR(–), 25% fall into the group DR(–)UACR(+), and 5% fall into the group of DR( + )UACR(+). In these outpatient populations, about 14% of DR(+) people showed significant differences in the measured value or positive rate of urine markers regardless of the development of retinopathy, suggesting that the occurrence of retinopathy and kidney damage in people with diabetes may not be closely associated with each other at least in certain patients. While some studies pointed out that DR and DKD might have been accompanied by and influenced each other [17, 18], our study showed a sizable portion of people with T2DM may develop the two conditions independently from each other.
Our second finding was that even in the patients having both negative values in DR and UACR, the positive detection rate of u-NAG/Cr reached 10.48%. It has been recognized that urinary NAG, which is located on the lysosome of renal tubular epithelial cells, can reflect the structural damage of renal tubular epithelial cells [19]. People with T2DM often have an elevated level of u-NAG/Cr possibly due to the overload burden of re-absorption, the local inflammation injury and hypoxia, etc. These conditions might happen before the glomerular damage. A previous study also showed that the u-NAG level was proportional to non-albumin proteinuria levels in T2DM patients with DKD even before the onset of overt albuminuria [20]. In the UACR positive group, the u-NAG/Cr positive rate was close to 40%, indicating that the effect of diabetes on the glomeruli and tubules was independent, rather than in concert, and varied from person to person. This finding strongly suggests that it is important to include renal tubular-related markers in the early screening of DKD. Further studies about the susceptibility of people with T2DM to glomerular or tubular injury are needed, and appropriate early intervention strategies also need further investigation.
Our third finding was that the positive rates of u-IgG/Cr were high even in the people with both negative values in DR and UACR. Previous research suggests that the increase in urinary IgG reflects the serious damage to the glomerular basement membrane [21]. The increase in a urinary IgG excretion rate seems to suggest a decrease in the estimated glomerular filtration rate (eGFR), which may be a marker of disease progression [22]. However, some other studies have reported that urinary IgG can rise before the occurrence of microalbuminuria or in normal albuminuria in people with diabetes [23,24,25], which is consistent with our results. It is possible that the increase in urinary IgG excretion may be due to selective damage to the glomerular pore size and increased intraglomerular water pressure caused by hyperglycemia [26]. As urine IgG has a higher sensitivity than that of microalbuminuria in reflecting changes in renal hemodynamics and inflammation [27], our finding suggests that urinary IgG can also be used as an early marker of diabetic kidney injury.
Our study also showed several abnormal increases in other urine proteins, including both glomerular and tubular relative biomarkers. The data shows that urinary renal tubular reabsorption biomarkers (such as u-α1MG/Cr, u-β2MG/Cr, u-RBP/Cr, and u-CysC/Cr) increased in the DR and UACR double negative group. This result suggests that the proximal tubule reabsorption function may be decreased in the early stage of diabetes, which can cause a large amount of low molecular weight proteins to be present in the urine [7]. The detection rates of tubular epithelial cell injury biomarkers (u-NGAL/Cr and u-NAG/Cr) were 4.03% and 10.48% respectively. The development of inflammation, stress, and increased reabsorption burden caused by high glucose could worsen renal tubular lesions. These biomarkers could help to evaluate the extent of renal tubular injury [28, 29]. The management and prognosis based on these biomarkers could be clinically significant and are worthy of further investigation.
We finally found that the positive rates for certain biomarkers did not show significant differences in patients having different years of diabetes. In both the group of diabetes with less than 5 years and other groups, it is observed that the top three biomarkers that have high positive rates were u-TRF/Cr, u-NAG/Cr, and u-IgG/Cr. This is true even in the DR(-)UACR (-) group. (See Fig. 3, Supplementary Fig. 1) As the onset of type 2 diabetes is difficult to pinpoint precisely, it is advisable to initiate annual testing for albuminuria and tubular injury markers at the time of diabetes diagnosis [16]. However, tubular markers might not have been frequently measured in the present clinical work, causing their clinical significance to be underappreciated to certain degrees. We suggest that different panels of tubular biomarkers should be used for diagnosing people living with T2DM at different diabetes duration for various purposes, to evaluate DKD more completely.
The study has several limitations. Firstly, it was a cross-sectional study that adopted continuous and convenient recruitment, and we provided the distribution of nine (9) urinary biomarkers only in people living with T2DM in a stable chronic condition. Secondly, due to limited conditions, we did not collect detailed medication information of the participants, such as their medication history. The eGFR and HbA1c results were collected for only a small number of participants. As a result, we were unable to thoroughly discuss any correlation among eGRF, HbA1c, and the results of nine (9) biomarkers in this study. Thirdly, we didn’t determine the range of the sample size for this study. When planning this study, we set up a minimum threshold and then tried to enroll as many participants as possible within the period. In addition, this is a single-center study.
In summary, diabetes retinopathy and renal lesions can be independent, and even a seemingly normal UACR could not rule out retinopathy. It is necessary to add renal tubule markers to the screening list of DKD, to fill in the gap in UACR-negative people living with T2DM. Early detection of renal tubular biomarkers is critical for adjusting treatment strategies, safeguarding kidney functions, and improving prognosis. Detection of both glomerular and tubule biomarkers is recommended in efforts to detect DKD in the early stages.


留言 (0)