Differences in Protein Structures
RSV is an enveloped virus with an RNA genome encoding a total of 11 proteins (reviewed in more detail in [13]). Four proteins associated with the membrane form the virus envelope: the matrix protein (M), the small hydrophobic protein (SH), the fusion protein (F), and the attachment glycoprotein (G). The virus genome protection and replication are mediated through the nucleoprotein (N), phosphoprotein (P), RNA polymerase (L), and the transcription processivity factor (M2-1). In addition, two nonstructural proteins (NS1 and NS2) are potentially involved in the escape strategy from infected cells.
The virus primarily mediates its viral attachment and entry into host cells via the attachment G protein and the fusion F protein that are on its surface. The interaction between RSV G and the host cell leads to the engagement of RSV F, which then drives fusion between the viral envelope and the host membrane. During fusion, RSV F undergoes a dynamic conformational change from a metastable prefusion trimer to a stable postfusion state. Over the years, as a result of their critical roles in mediating attachment and fusion, and the induction of the majority of neutralizing antibodies in vivo, RSV G and F were the best-studied proteins.
RSV A and RSV B Subgroups are Established by RSV G Antigenic and Sequence Variations
The RSV G is the most variable RSV gene sequence and is used to define RSV genetic variants [14]. RSV is classified into two major subgroups, RSV A and RSV B, initially based on antigenic differences using G protein-specific mAbs [15, 16]. Within each of these two subgroups, several genotypes have been further identified and described. Although there are no criteria for genotype definitions that reach consensus, 15 distinct genotypes have been described for RSV B [17] and nine distinct genotypes for RSV A [18] (Table 1).
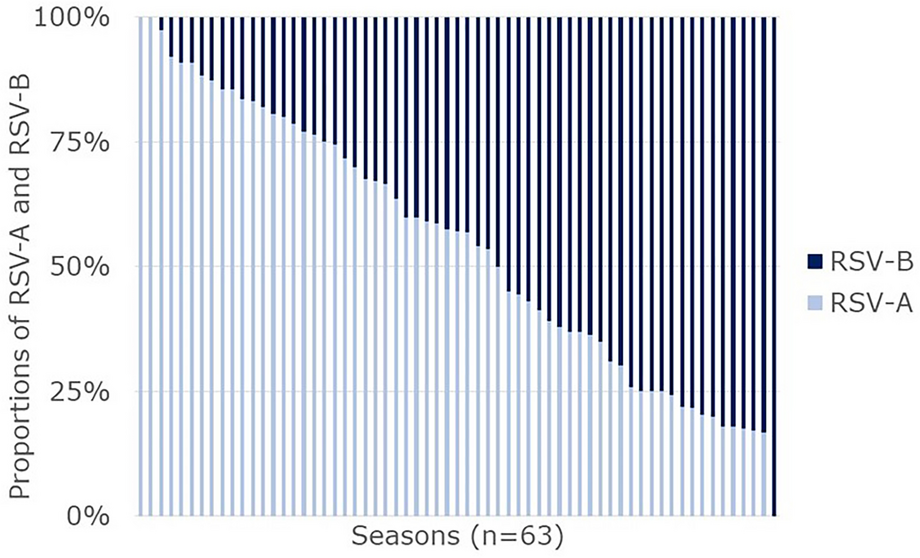
Table 1 RSV A and RSV B genotypesRSV keeps evolving worldwide and new genotypes emerged over the years. The genotypic diversity within RSV B is greater than within RSV A (see Table 1). While RSV A strains can be grouped into seven distinct genotypes, at least 37 RSV B genotypes have been described [17], of which only the most dominant ones are listed in Table 1. This is most likely due to RSV B having a higher genome-wide evolutionary rate than RSV A (higher number of substitutions per site per year) [19, 20]. However, strikingly, a recent phylogenetic analysis of the Global Initiative for Sharing All Influenza Data (GISAID) database suggests that the nucleotide diversity in the G protein is three times higher in RSV A than in RSV B [21]. In recent years, several genetic modifications in RSV G have been identified. In the RSV A subgroup, a 72-nucleotide duplication is observed (referred to as the Ontario 1 (ON1) lineage), whereas in the RSV B subgroup, a 60-nucleotide duplication is observed (referred to as the Buenos Aires (BA) genotype) [22, 23]. Although there is still debate on whether they can be considered as new distinct genotypes, both became predominant circulating strains. Genotype diversity decreased over the last two decades, and ON1 and BA9 have become the sole lineages detected for RSV A and RSV B [24,25,26,27,28,29,30,31,32,33]. Whether the G gene duplication plays a role in the predominance of the ON1 and BA9 remains an open question [20]. There is only limited in vitro data suggesting improved infectivity with the duplication and no clinical evidence so far [34].
RSV F, More Conserved Among RSV A and RSV B, is a Major Target for Vaccine and Monoclonal Antibody Development
RSV F is evolutionarily more conserved than RSV G and as such serves as a common therapeutic target for both RSV A and RSV B subgroup viruses. RSV F differs by only 25 amino acids between RSV A and B [35]. The structure of RSV F in prefusion conformation was solved in 2013 and is guiding new vaccine development approaches [36].
F contains antigenic sites that are both shared by the prefusion and postfusion conformation and sites that are unique to each conformation. Six major antigenic sites have been defined on the RSV F (Ø, I, II, III, IV, V). Some antigenic sites are expressed on both pre-F and post-F, while other sites are presented on only one conformation (see Table 2). The antigenic sites I, II, III, and IV are present in both the pre- and post-F conformation and present different binding affinities; at one end of the spectrum, antibodies targeting site I show a preference for post-F and low neutralizing activity, while at the other end of the spectrum, those targeting site III show a preference for pre-F and have relatively potent neutralizing activities. The antigenic sites Ø and V are only displayed in the pre-F conformation of RSV F and present the highest binding affinity for neutralizing antibodies (see Table 2) [37,38,39].
Table 2 Antigenic site-specific antibodies elicited by pre-F or post-F antigens and neutralizing potencyAlmost 50% of the most potent neutralizing antibodies are targeting the pre-F-specific site V in recently studied healthy adults [40]. Importantly, pre-F has been proposed as a superior vaccine candidate since antibodies bind antigenic sites Ø and V with high affinity [41].
Even though the RSV F is relatively well conserved, it evolves continuously. Over time, changes in the amino acid sequence have been observed. Some of these changes led to differences in F antigenic sites compared to reference F sequences (e.g., RSV/A Long strain), which are more pronounced in antigenic sites of the prefusion conformation of RSV B [11, 42]. Data from the INFORM-RSV 2017–2018 pilot season were crucial to establish a molecular baseline of RSV F sequence and antigenic site variation. This can be used to track frequency, geography, and evolutionary trajectory of potential neutralization escape variants, providing an evaluation system for ongoing development of vaccines and mAbs [33]. Despite low variability in the 2017–2018 RSV F sequences, new variants constantly emerge in some regions, which suggests positive selection pressure. Indeed, in a study from China (2014–2016), multiple amino acid differences were found for RSV F, located at multiple antigenic sites, varying between RSV A and RSV B [43]. In a study in the USA (2015–2019), changes at the F antigenic sites of RSV B were more frequent than RSV A, mainly occurring at antigenic sites V (99.6%), Ø (18.6%), and IV (7%) of RSV-B F [44]. In another study in China, the RSV F amino acid sequence homology between RSV A and RSV B was 89–90.6%, with more mutations found in antigenic site II, a target site for mAbs [45].
Subgroups and ImmunityNeutralizing Antibodies: RSV A RSV B Cross-Reactivity
The RSV neutralizing activity in human sera is primarily derived from antibodies targeting the F protein in its prefusion conformation (pre-F specific antibodies), and more specifically antigenic sites Ø and V [38, 40]. Immunological analysis demonstrated that more than 85% of highly potent antibodies were specific for prefusion F. Furthermore, pre-F specific antibodies were more potent than pre- and post-F cross-reactive antibodies and also more potent than specific post-F antibodies; hence, the interest to target prefusion conformation [38]. In contrast, virus neutralization was not observed with G-specific serum [46]. Consequently, most current monoclonal antibody and vaccine design efforts are focused on RSV F.
The majority of neutralizing antibodies induced by natural infection on adults showed activity against both subgroups A and B [38]. They neutralize a diverse panel of clinical isolates and demonstrate in vivo protection. Such studies confirm that the prefusion F has highly conserved epitopes and is therefore a desirable target for RSV vaccines and mAbs [47]. However, some studies have shown that numerous antibodies targeting site Ø had more neutralizing potency toward RSV A than toward the RSV B [41].
Studies evaluating the human antibody response to RSV F in adults following natural infection, who have likely been exposed to RSV A and RSV B, have shown that most anti-RSV F mAbs are subgroup cross-reactive. Very occasionally, mAbs are found that appear to be subgroup-specific or subgroup-preferring [12, 38].
MAbs targeting site Ø showed the most variations in neutralization potencies between the two different RSV subgroups. Some mAbs directed at RSV A site Ø present no or less neutralization activity against RSV B. Indeed, two site Ø-specific mAbs have been well characterized: 5C4 and D25. They recognize antigenic site Ø but at different angles. 5C4 potently neutralizes a panel of RSV A subgroup strains but has limited neutralization activity against subgroup RSV B strains. In contrast, D25 potently neutralizes strains of both RSV subgroups. D25 is a mAb that has been isolated from human B cells derived from an adult most probably infected throughout life with RSV strains of both RSV A and B subgroups [12]. These results show the existence of differences in binding of neutralizing antibodies to key RSV epitopes such as the antigenic site Ø, which can yield neutralization of both RSV subgroups or only a single subgroup.
Finally, clinical proof of concept for prefusion F vaccine design came from immunogenicity data of phase I clinical trial showing a booster effect in neutralizing activity in serum. These findings suggest that developing a successful RSV vaccine is feasible. The boost in neutralizing activity toward subgroup B after immunization with a subgroup A F vaccine shows the high conservation of F between subgroups, and immunity acquired most probably from multiple prior infections by both RSV A and B subgroups [48, 49].
It remains difficult to study the genotype-specific immune response in human cohorts, due to diversity in the hosts, which makes it hard to assign differences to pathogen diversity alone. For instance, when the innate immune response was studied by analyzing the expression level of interferon (IFN)-related genes in infants with RSV bronchiolitis, it was shown that induced interferons (IFN)-stimulated genes (ISGs) differed between patients infected with different genotypes [50]. Furthermore, these ISG expression levels were associated with severity in bronchiolitis clinical manifestations; ISGs expression level was lower in ON1- and BA- than in the NA1-infected patients. The lineage ON1 demonstrated a high replicative capacity but seemed to be clinically less severe than the previously circulating RSV A, NA1. But whether the ISG downregulation in ON1-infected infants is a consequence or a cause of high viral load increase remains to be established [50].
Cellular Immune Response
While inducing potent neutralizing antibodies is the primary objective in most vaccine development programs, both CD4 and CD8 T cells play a key role in the clearance of infected cells and hence the protection against RSV infection [51].
Amino acid variation and the appearance of novel epitopes on RSV proteins of recent circulating RSV strains have been described [43]. Using a computational approach, RSV surface proteins were predicted to have a strong potential to elicit T cell immunity, with the F protein potentially having a high T cell epitope density [52]. Computational results suggest that RSV surface proteins may stimulate T cells that are essential for protective immunity. However, some epitopes were mutated in some strains. The percentage of conserved T cell epitopes in the RSV F protein when comparing the vaccine and corresponding wild type strains is substantially similar in the two subgroups. The proportion of conserved epitopes was higher than 78% for RSV A and higher than 85% for RSV B [52].
Polyfunctionality refers to the ability of T cells to perform a range of functions, including the secretion of cytokines, chemokines, or cytotoxic granules simultaneously at the single-cell level. The presence of polyfunctional T cells could be a sign of immunological disease control; their role in RSV protective immunity is unknown. Blunck et al. [53] found that, in healthy adults under the age of 65, both the acutely and recently RSV-infected groups had lower T cell polyfunctionality, for both CD4+ and CD8+ memory T cells, than the uninfected group at enrollment. The uninfected group was defined as adults who remained uninfected through the season. This suggests that the presence of polyfunctional RSV-specific memory T cells may protect against re-infection. More importantly, while RSV B was the dominant circulating subgroup during the study period, and stronger neutralizing antibody responses were observed against RSV B than against RSV A, polyfunctionality across all T cell subsets was higher after exposure to RSV-A F than RSV-B F protein peptide libraries. It is unclear whether this difference in response is reflective of what these adults were primed with in prior respiratory seasons. The authors conclude that “bivalent vaccines containing both RSV subgroup antigens may be warranted, at least for the older adult population” [53].
Monoclonal Antibodies: Cross-Reactivity Between RSV A and RSV B
Studies on crystal structures have shown that the antigenic site Ø presents various conformations and that even though individual mAbs may have preferential binding affinities to a specific subgroup, the antibody epitopes overlap substantially between RSV A and RSV B [54]. However, site Ø is the most variable surface epitope between RSV A and RSV B.
The anti-RSV fusion protein mAb nirsevimab received marketing authorization from the European Medicines Agency (EMA; October 2022) and US Food and Drug Administration (FDA; July 2023). This mAb binds the prefusion RSV fusion protein at a conserved discontinuous neutralizing epitope in site Ø. It blocks viral entry into host cells and a single dose confers protection for 5 months [55, 56]. However, decreased susceptibility to nirsevimab does occur, as observed in the randomized clinical trial, where two RSV B clinical isolates were identified in the study arm, that had decreased susceptibility to nirsevimab [57]. In a study of 322 samples from three European countries [58] conducted before the nirsevimab approval, isolates collected from 0.8% of the immunoprophylaxis-naïve participants were found to contain a nirsevimab resistance-associated substitution. Similarly, using nearly 6000 RSV-positive nasal samples from 17 countries, another study assessed the frequency of mutations and evaluated the effect of these mutations on the in vitro potency of nirsevimab neutralization [59]. Only one mutation in RSV A, Lys68Glu, resulted in a tenfold or higher change in the inhibitory concentration. Four mutations in RSV B, Lys68Asn, Lys68Gln, Asn201Ser, and Asn201Thr, resulted in a tenfold or higher change in the inhibitory concentration. Each of these binding-site substitutions was rare (< 1%) in circulating RSVs between 2015 and 2021 [59]. Following the introduction of nirsevimab, it is unclear whether its broad use could lead to selection of these resistant viruses over time [33].
Suptavumab, a monoclonal antibody which binds antigenic site V, a conserved epitope on both RSV A and RSV B subgroups, was tested in healthy infants. In a phase III trial, isolated RSV A virus had no suptavumab epitope changes while all isolated RSV B virus had a two-amino acid escape mutation in the suptavumab epitope. This substitution on this newly circulating mutant strain of RSV B led to complete loss of neutralization antibody activity; as a result, suptavumab did not meet its primary efficacy endpoint [60].
Clesrovimab, a monoclonal antibody currently in a phase III trial, binds to RSV F site IV [47, 61]. Site IV is relatively well conserved between RSV A and RSV B [11, 42], and is more conserved than sites Ø and V [47]. Site Ø and V reside at the top half of the RSV prefusion F trimer in contrast to site IV, which resides on the lower half of the prefusion F trimer. This may make site IV mAbs less vulnerable to evolutionary pressure [42]. However further evaluation will be required as other studies have shown variation in site IV of the RSV B subgroup [44].
The current data with these three mAbs shows that close surveillance will be necessary to follow the emergence of mutated RSV strains that could impact the efficacy of mAbs. It also suggests that in the absence of immune pressure, a polyclonal vaccine response is anticipated to be less vulnerable than mAbs to RSV F surface amino acid substitutions, particularly those targeting antigenic site Ø. As mAbs target a single epitope, these may be more prone to drive immune escape compared to a polyclonal vaccine response.
Clinical Course of Infection, and Severity Outcomes
RSV can cause a range of symptoms from a mild cold to a serious respiratory illness. Complications are similar to those caused by influenza and other respiratory viruses, and can include pneumonia, cardiopulmonary complications, intensive care unit (ICU) admission, the need for mechanical ventilation, and might lead to death.
RSV surveillance is essential to improve our understanding of RSV incidence and diversity. Yet, currently, we do not fully understand how this diversity impacts clinical outcomes. A comprehensive collection of papers reporting on the impact of RSV subgroup on clinical severity is shown in Table S1 in the electronic supplementary material.
Two studies, performed in West Virginia, showed that the clinical categorization of the illnesses associated with subgroup A and subgroup B strains appeared to differ between the two subgroups. Bronchiolitis occurred at a lower frequency in children with RSV B (p = 0.025), whereas croup occurred more often (p value not reported) [62, 63]. Similar results were obtained in a study from Finland, where bronchiolitis was observed in 71% of children with group A infection and 59% of children with group B infection (relative risk 1.21; confidence interval 1.02–1.43; p = 0.02) [64]. However, using previously described diagnostic criteria [62, 63], these findings could not be verified in a Japanese study population [65].
Out of 46 studies reporting RSV subgroup impact on clinical severity, 29 studies reported no significant differences in severity between subgroups A and B [9, 65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,



留言 (0)