The results of this study present the similarities and differences in the healthcare settings, clinical presentation, treatment practices, and treatment response of patients with NTM-PD in Japan and the Eur5. Furthermore, the findings bring to light the treatment practices that may result in poor prognosis for patients with NTM-PD in Japan and the Eur5, such as delay in treatment initiation, lack of treatment, prescription patterns of antibiotics, reliance on symptomatic improvement as a criterion for stopping treatment, and the potential lack of adequate consideration of culture conversion status. A lower percentage of physicians in Japan were “entirely satisfied” with their patients’ treatment outcomes than physicians in the Eur5. These insights can help in re-evaluating and improving the diagnostic and management strategies for NTM-PD used by physicians in Japan and the Eur5.
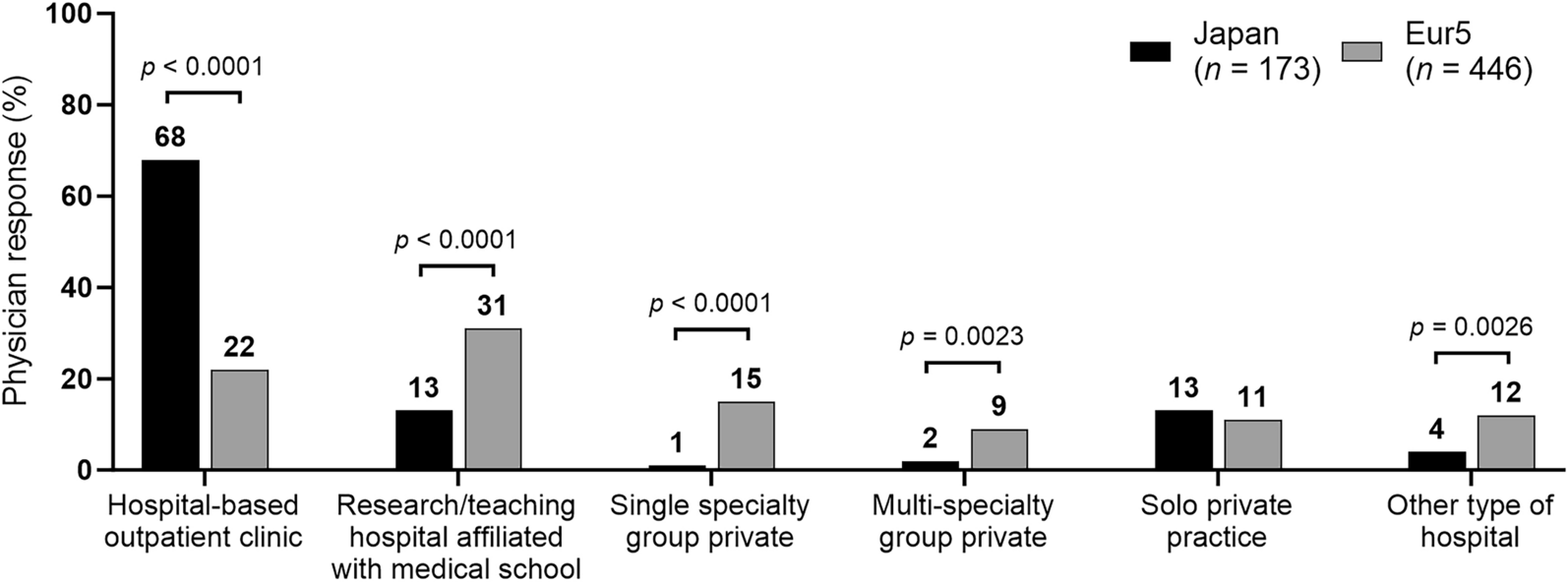
Cultural differences between Japan and the Eur5 could influence clinical patterns and the approach to disease management, which could impact treatment outcomes. Patients with NTM-PD were predominantly treated in NTM-PD speciality centers in a community setting in Japan compared with those treated in an academic setting in the Eur5, which may lead to longer and more frequent physician assessment. This might be caused by the historical background of the medical system in these countries. For example, in Japan, national hospital organizations based on tuberculosis sanatorium and treatment centers have contributed substantially to the care of patients with respiratory diseases, including NTM-PD; prior to the 1990s, most clinical studies and epidemiologic analyses of NTM-PD were conducted by national hospital organizations [13, 14]. Because of the increasing prevalence of NTM-PD, academic hospitals have also been treating and studying this respiratory disease in recent years. Furthermore, annual health check-ups, which are common in Japan, could play a role in the early diagnosis of mild cases and treatment in a community setting [15]. By contrast, more severe cases observed in the Eur5 were treated in an academic setting. Treatment practices for patients with NTM-PD could differ between speciality, academic and non-speciality centers; therefore, the management gaps between the providers in these settings should be assessed. The lower prescription rate of concomitant medications such as β2-agonists, inhaled combination steroids, oral steroids, and anti-reflux therapy in Japan than in the Eur5 may be because asthma and gastroesophageal reflux disease were reported in a lower percentage of patients with NTM-PD in Japan than in the Eur5 (7% vs. 17% and 6% vs. 11%, respectively). There is a need for an integrated NTM-PD management beyond antimicrobial therapy, which includes managing comorbidities and implementing a personalized pulmonary rehabilitation plan and airway clearance techniques to improve symptoms, exercise capacity, and health-related quality of life [16]. Moreover, a multi-disciplinary approach would further improve the management of NTM-PD in addition to that achieved using drug therapy [17].
A limitation to this study is that the survey did not collect data in a way that confirms if patients were prescribed a guideline recommended three-drug regimen, which makes it difficult to compare physicians’ adherence to guideline-based prescribing. In a population-based cross-sectional study conducted in Japan, 30.8% of patients received standard treatment [e.g., (1) macrolide, rifamycin, and ethambutol; (2) macrolide and ethambutol], 37.3% received non-standard treatment [e.g., (1) only macrolides, (2) macrolides and rifamycin, or (3) macrolides and fluoroquinolone], and 31.9% received no treatment [18]. In this study clarithromycin was prescribed more commonly than azithromycin in both the Eur5 and Japan. Although this is not consistent with the 2020 guidelines for NTM-PD, which recommend azithromycin over clarithromycin as part of the multidrug regimen for treatment in macrolide-susceptible MAC-PD [19], at the time the study was conducted in 2013 the guidelines available (from 2007) did not state a preference [10]. In addition, clarithromycin was the only guideline that recommended macrolide with an indication that was covered by Japan’s national insurance program in 2013. With 85% of NTM-PD cases in Japan reported to be MAC-PD, this could explain the lower use of azithromycin in Japan versus the Eur5 in this study.
Although the study was conducted before the 2020 guidelines for NTM-PD were published [19], the survey results revealed that there were deviations from the 2007 recommendation [10] in real-world clinical practice in Japan and the Eur5. Patients with good overall health, mild symptoms, and awaiting results for antimicrobial susceptibility testing and other laboratory tests were the main reasons for the lack of or delay in therapy initiation in Japan and the Eur5 in this study. In our previous publication, the variables influencing the treatment decision in patients with NTM-PD in Japan and the Eur5 were determined [8]. Patients assessed by their physician to have moderate or severe symptoms at presentation and those aged > 60 years, living in Spain and Italy, having sputum specimens for acid-fast bacilli analysis being used for diagnosis, having fever as a symptom at the first presentation, and having poor/very poor or fair physician-based rating of overall health were also more likely to be treated [8]. The smaller proportion of patients starting treatment in Japan versus the Eur5 is notable and may be due to differences in disease severity between the two populations. As reported previously, in this survey most patients in Japan were considered by their physicians to have mild disease, whereas most patients in the Eur5 had moderate or severe disease [8]. At the same time, patients in Japan may have been perceived to have less severe disease and, as a result, experienced a delay in treatment initiation, which is understood as a watchful waiting strategy. The perception by Japanese doctors was that the more limited radiographic improvement and smaller proportion of patients experiencing culture conversion might be due to deviation from the standard treatment and frequent recurrences, which have not been noticed in clinical practices. A significantly larger proportion of patients in the Eur5 were prescribed linezolid and moxifloxacin compared with Japan. In European and US guidelines, clofazimine, moxifloxacin, and linezolid have been described as regimen options for resistant refractory NTM-PD with cavitation. In Japan, these antibiotics are not reimbursed by insurance, and the 2012 Japanese NTM-PD treatment guidelines did not include regimen options for such cases, which might explain the discrepancies in the use of these antibiotics between Japan and the Eur5.
Symptom-based NTM-PD management could lead to more advanced diseases, such as cavitary lesions, severe bronchiectasis, and increased bacterial load (as measured by time-to-positivity of the mycobacteria growth indicator tube automated broth culture system) [20], which are associated with poorer outcomes and more cases of refractory disease. Therefore, regular radiology and sputum examinations are warranted for the decision of initiating treatment, provided that these risk factors for refractory outcomes are not already present at the first diagnosis, leading to immediate treatment recommendation and consideration of treatment intensification [19, 21]. Moreover, symptomatic improvement was the most common treatment goal. The optimal treatment duration, as defined by current guidelines published after these data were collected, for NTM-PD is defined as ≥ 12 consecutive months during which culture negativity is maintained [19]. A paucity of studies and differences in patient characteristics, practice settings, and resources hinder the establishment of an optimal treatment duration for NTM-PD [19]; however, two studies have indicated that the treatment duration could change based on disease severity as determined by radiologic evaluation [22, 23]. Nevertheless, symptomatic worsening is associated with treatment initiation and poorer health-related quality of life; for patients who achieve microbiologic conversion, health-related quality of life and survival are improved, highlighting the importance of culture conversion as a treatment goal [24, 25]. Educational initiatives to increase guideline-based therapy, particularly regarding culture conversion, could improve the treatment success rate and lower the relapse rate, ultimately leading to reduced patient mortality.
Overall, the percentage of patients in Japan who had a “greatly improved” status on the most recent radiologic test was half of that in the Eur5. However, patients in Japan may have had less potential to show great improvement as they were generally diagnosed at an earlier disease stage than those in the Eur5. Poor prognosis on radiologic examination and a higher number of refractory patients in Japan than in the Eur5 may be the reasons for a lower percentage of physicians in Japan being “entirely” satisfied with the treatment outcomes than that in the Eur5 (19% vs. 43%). The high rate of refractory NTM-PD in Japan may be due to the use of a substandard treatment regimen, including a shorter than recommended duration of treatment (59% of patients received treatment for > 6 months and 41% received treatment for > 1 year) and the administration of a macrolide without ethambutol or rifampicin [11]. Of note, the nodular-bronchiectatic form is more common in Japan than in the Eur5 [8], which may result in increased rates of reinfection in patients in Japan during and after treatment, similar to that reported in the US [26]. Knowledge sharing and increasing the awareness of guideline recommendations regarding the management of NTM-PD, as well as a systematic treatment approach, are essential for improving the current situation.
An important limitation of this study is that the survey was completed before the release of the latest guideline recommendations in 2020; hence, the analysis was based on the 2007 guideline recommendations for NTM-PD [10]. However, this being the only study of its kind and size conducted in Japan and the Eur5 to date, the findings are relevant even today. Adherence to guidelines in Japan and the Eur5 was assessed based on the prescription data of individual antimicrobials instead of their drug class (e.g., macrolides) or the three-drug regimen for MAC-PD; however, the percentage of patients receiving the individual drugs could serve as an accurate reflection of adherence. Another limitation of the survey is the lack of data on antimicrobial sensitivity, which may have provided further insights into the differences in prescribing patterns between Japan and the Eur5. As patients in the Eur5 had a higher prevalence of asthma, it is possible that respiratory symptoms due to underlying airway disease could be mistaken for symptoms of NTM-PD. Other limitations include potential self-report bias because physicians or their designated personnel retrieved and input the survey response data themselves into an online survey instrument and a lack of uniform susceptibility testing as well as insights into the varying patterns of antibiotic prescriptions across diverse populations.



留言 (0)