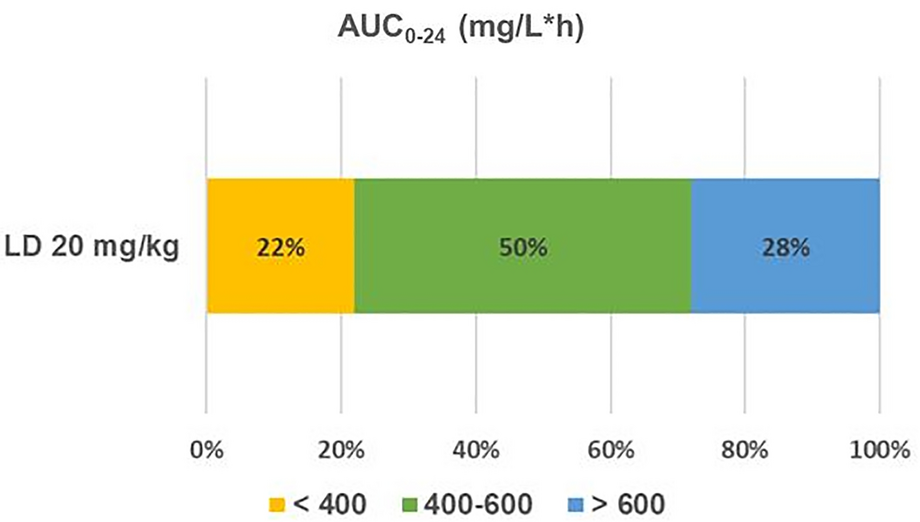
In this study, we investigated the impact of a fixed VAN LD on the AUC0–24 using a non-trapezoidal linear PK approach. We found that only 50% (61/123) of patients who received 20 mg/kg VAN LD achieved the target AUC0–24 of 400–600 mg/l*h, while the remaining 50% (62/123) were either subtherapeutic or supratherapeutic.
Patients in the subtherapeutic cohort exhibited a faster Ke, increased VAN clearance, and larger Vd. These differences can potentially be attributed to the combined effects of younger age and increased body weight, impacting VAN PK [21,22,23]. Specifically, both youth and increased body weight are known to correlate with enhanced VAN clearance, as supported by existing literature [1, 21, 23, 24]. Our findings align with this observation, as VAN clearance in our cohort was higher than that reported in the general population (8 vs. 5 l/h) and more consistent with VAN clearance reported in younger patients with obesity (8 vs. 6–10 l/h) [5, 21, 25]. Conversely, since increased body weight and youth have opposing effects on VAN Vd, this parameter had less impact on VAN disposition in this young cohort with obesity [21,22,23,24]. It is essential to note that VAN Vd does not scale proportionally with actual body weight, underscoring the importance of limiting the LD to mitigate the risk of toxicity [2, 21, 22, 26]. Given that VAN clearance was the primary determinant of underexposure in this cohort, shortening the dosing interval of the maintenance dose rather than increasing the total LD may be a more prudent approach to optimize exposure (\(Maintenance dose = Clearance \times Concentration \times Dosing interval\)) [5].
In the supratherapeutic cohort, patients exhibited lower Ke and VAN clearance, which can potentially be attributed to the combination of older age and poor renal function at baseline. The median age of these patients was 64 years old (IQR 42, 77), with 23% (8/35) of patients having CKD at baseline. Matzke et al. conducted a study investigating the relationship between changes in renal function and VAN PK across different age groups [27]. They employed linear PK equations to characterize VAN disposition after the first dose, similar to the methodology employed in this study. The authors reported a significant decrease in VAN clearance (2.4 l/h) and Ke (0.05 1/h) in patients aged between 46 and 66 years old and creatinine clearance (CrCl) between 40 and 87 ml/min. Similar to the results of these findings, our cohort’s median (IQR) VAN clearance and Ke were 3 l/h [2, 4] and 0.06 1/h (0.03, 0.07), respectively. The author concluded that reduced renal function was associated with a marked impact of VAN clearance, and dosage adjustment is warranted [27]. Since the Vd in this cohort was similar to values reported in the literature (0.7 l/kg), a change in LD is not required. Instead, extending the dosing interval may be a more effective solution to optimize exposure and minimize nephrotoxicity [5].
In our study, a 20 mg/kg LD resulted in a median AUC0–24 of 525 mg/l*h, and achieved AUC > 400 mg/l*h in 78% (96/123) of the patients. Prior research by Hosiamont et al. and Pongchaidecha et al. proposed a higher LD of 25–30 mg/kg to optimize VAN AUC0–24 [8, 9]. However, both studies focused on patients admitted to the ICU, where a higher LD might be warranted. A LD of 25–30 mg/kg resulted in AUC0–24 > 600 mg/l*h in over 50% of patients in both studies [8, 9]. The majority of the patients included in our study did not require an ICU admission (73%, 90/123). Notably, our study excluded a small cohort of critically ill individuals with a subtherapeutic serum vancomycin concentration after receiving a LD of 20 mg/kg. It is unclear whether a higher dose of 25 mg/kg would have been more beneficial for these patients. Importantly, we observed a lower incidence of AKI compared to the findings reported by Hosiamount et al. (14 vs. 38%) [8]. Although the causation between VAN LD and nephrotoxicity remains uncertain, an AUC0–48 > 650 mg/l*h was associated with an increased risk for AKI [28]. Future research should further explore the appropriate dose for the critically ill versus non-critically ill population. Otherwise, a 20 mg/kg LD appears sufficient to optimize VAN exposure without increasing the risk of nephrotoxicity in patients not admitted to the ICU.
Most studies evaluating the impact of a VAN LD on AUC0–24 utilized Bayesian software to estimate AUC0–24. While Bayesian software provides reliable AUC estimates, cost and clinical experience can limit their implementation [29]. According to a 2019 survey aimed at assessing VAN monitoring practices in academic medical centers in the U.S., 23% (18/78) of surveyed institutions performed AUC-based monitoring. Only 28% (5/18) of institutions have implemented Bayesian software, while 67% (12/18) used linear PK equations for AUC estimation [30]. Bayesian software can potentially underestimate the true AUC by 14% to 23%, depending on the PK model and sampling strategies [31]. In this study, we employed non-trapezoidal linear PK equations to calculate AUC0–24. The main advantages of this method are simplicity, accessibility, and generalizability. Linear PK equations can be incorporated into electronic medical records and applied routinely in clinical practice [17]. By using timed post-distribution peak and trough levels to calculate patient-specific PK parameters (Vd and VAN clearance) and AUC0–24, fewer assumptions were made, resulting in a more accurate estimation of the true AUC [1, 7, 11, 32].
For simplicity, we used VAN total daily dose (TDD) and calculated VAN total body clearance to estimate AUC0–24 (\(AUC=\frac)\)[1, 11, 12, 14]. This approach captures the true AUC0–24 associated with the total VAN dose administered within the initial 24 h of therapy (i.e., LD ± maintenance doses). Given that VAN disposition can be described using one-compartment mono-exponential equations, provided two levels are collected during the elimination phase, VAN clearance was determined using compartmental approaches (\(VAN clearance=K \times V\)) [5, 33]. However, when applying one-compartment equations to drugs with two-compartment dispositions like VAN, drug loss during infusion (α-phase) is not fully accounted for, resulting in a slight underestimation of the true AUC [6]. Yet, intermittent infusion equations were used to account for most drug loss during infusion, which is likely insignificant as the median VAN half-life was five times longer than the infusion time [5, 7, 34]. Furthermore, 78% (96/123) of patients achieved an AUC0–24 > 400 mg/l*h. Even if the true AUC was slightly higher than what was estimated by this approach, this finding does not alter the conclusion that a LD of 20 mg/kg would suffice to optimize VAN exposure within the initial 24 h of therapy for the majority of non-critically ill patients with good renal function.
This study has several strengths, including the use of the specific AUC0–24 values for each patient allowing for minimal assumptions and improved internal validity as well as including patients with varying acuity of illness (27% of the patients were with critical illness) and PK profiles (50% of the patients were with obesity), thereby increasing the study's external validity. Despite the strengths of the study, this study has several limitations that warrant consideration. Firstly, due to the limited study period, our study did not include patients with a BMI below 18.5 kg/m2. Although VAN dosing is weight-based and adjusts for differences in body weight, it has been suggested that VAN’s Vd may not scale proportionally with actual body weight. Further investigation is needed to understand the impact of a 20 mg/kg LD of VAN on this population, as well as on other special populations not well represented in our study.
Secondly, the retrospective design of the study limited our ability to establish causality. Additionally, the small number of subtherapeutic and supratherapeutic patients prevented us from performing robust statistical analyses. Future studies with larger populations should aim to determine whether the variables identified in this study show significant correlations. Finally, the target AUC range of 400–600 mg*h/l is primarily validated in severe MRSA infections. In this study, only 26/123 patients (21%) had confirmed MRSA infection. However, this study focused on describing how fixed VAN LD affects AUC0–24. The clinical implications of achieving the AUC target for non-MRSA infections require further investigations.



留言 (0)