
記住我


During the second and third semesters of the ten-semester medical training programme at the UFS, students receive lectures and assessments on epidemiology, biostatistics, and the research process (Table 1). In semesters 2 to 5, students (in small groups established by themselves) go through the research process, from protocol planning and ethics submission to reporting their research findings, under the guidance of a medical or scientist supervisor from a clinical or laboratory discipline. Supervisors take part on a voluntary basis and student project groups are allocated to a supervisor in a specific field based on the preference for a study area indicated by the project group. Project groups and supervisors (ideally) discuss potential research ideas to finalise the topic. Module leaders monitor progress throughout and provide support when required.
Table 1 Undergraduate medical student research projects: main activities per semesterIn the initial years (with class sizes of 70 to 90), students could work on projects individually or in pairs but with increasing class sizes, the number of students per project group was increased to 3 to 4, and is currently 6 to 8 students (current class size 160 to 180 students). To enhance project viability, students who have to repeat an academic year but have passed the research modules continue with their projects as planned. Group marks are allocated for the protocol, presentation and final report. Students may choose to write individual reports. At the project presentations (where one speaker chosen by the group presents on behalf of the group), the module team acts as adjudication panel and students assess the presentation of other project groups.
The module team has annual planning sessions to discuss student feedback and module issues and consider possible changes to the modules. Refinements that have been implemented over time when the need was identified by the module team included:
Clarifying the role and responsibilities of supervisors to try to ensure some uniformity regarding supervision approaches;
Encouraging supervisors to attend project discussion sessions between project groups and the module team to keep all involved in the project informed;
Clarifying expectations and guidelines for students and supervisors regarding the format, content and assessment of the protocol, presentation and report to ensure uniformity;
A set amount available from the School of Medicine Research Committee for project funding to prevent costs from hampering some students’ ability to perform their project;
A formal session where student groups present their project topics to the module team and supervisors early in the planning phase to ensure that all involved have an early opportunity to comment on and guide the planning;
Supervisors keeping a register of attendance of meetings with the project group and the module team subtracting marks for students for non-attendance to promote student participation;
Allocating marks for draft protocols that project groups submit to the module team for feedback to ensure that students apply their minds and do not rely only on the feedback;
Providing general feedback online to the class after the project presentations to enable changes to the project reports that are submitted 2–4 weeks later;
Expecting students to write individual abstracts and conclusions for the research report to incorporate some individual work in what mainly is a group activity; and
Increasing practical sessions regarding administrative aspects of, for example, the ethics application and documentation to ensure that these aspects do not cause time delays and uncertainty.
Changes that have been attempted over the years but abandoned included the following:
A block set aside in the programme for students to perform data collection—it was found that not all projects allowed for data collection in the same time period.
Students assessing group member activity and group marks adjusted accordingly for individual students—it was found that group members varied in their assessment and there were frequently mitigating circumstances why a specific group member did not participate at certain stages of the research process.
Discussion meetings of all supervisors with the module team—finding appropriate time slots was difficult. Supervisors are reminded and encouraged to contact module leaders as needed.
Formal written feedback from supervisors regarding their experiences—most supervisors preferred to give informal feedback when they happened to see the module leaders in the corridors.
A feedback session with the class after reports had been marked—this was usually close to exam time and it was difficult to find an appropriate slot on the semester planner. Project groups can, however, contact the module leaders for feedback.
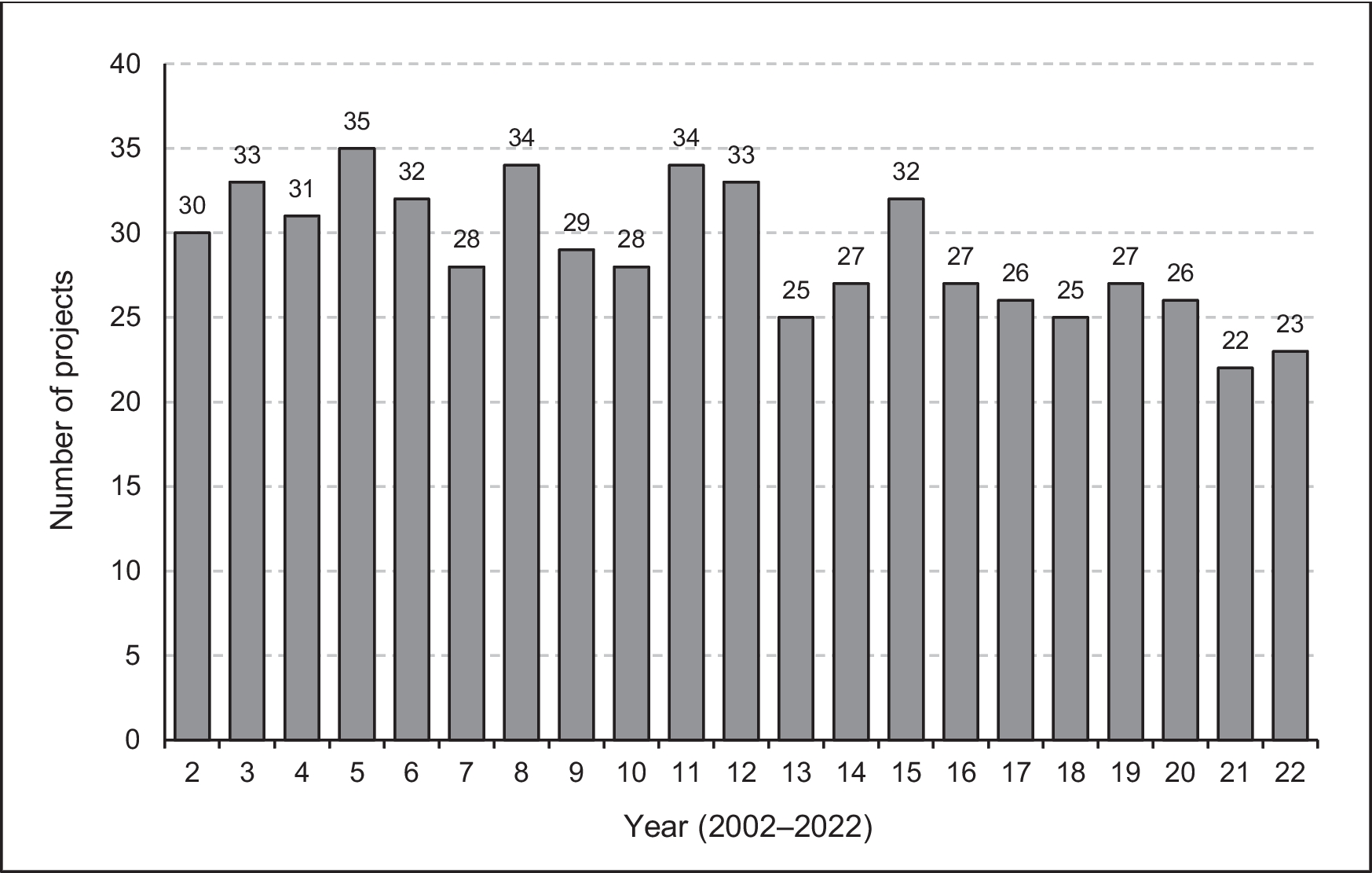
ProjectsDuring the study period, 607 projects were planned with the number per year ranging from 22 (in 2021) to 35 (in 2005), as shown in Fig. 1.
Fig. 1
Number of undergraduate medical student projects annually (n = 607)
Thirty-nine faculty departments/divisions/units were involved in supervision; the top five in terms of the number of groups supervised were the Departments of Family Medicine (86 project groups), Paediatrics and Child Health (66), Internal Medicine (64), Obstetrics and Gynaecology (47), and Psychiatry (44). These supervisors were all medical clinicians or clinical psychologists. Three departments, namely Family Medicine, Paediatrics and Child Health, and Internal Medicine, were in the top five in each of the three time periods, with Family Medicine supervising 23.9% (42/176) of the projects in the period 2016–2022.
Two hundred and twenty-nine supervisors (of whom six were in private practice) guided students, with nine supervisors guiding at least ten groups. One supervisor guided 19 groups (one each in 19 of the 21 year groups). Fourteen supervisors had completed these undergraduate research modules as part of their own undergraduate training. For 17 (2.8%) projects, supervisors preferred to work in a team of two (15 projects) or three (two projects) co-supervisors. For 24 (4.0%) projects, the supervisor was guiding more than one project group in the same year group. For 15 (2.5%) projects, supervisors needed to be replaced due to moving away (n = 7) or not fulfilling their supervisory duties (n = 8).
Given the wide range of departments involved in supervision, the research themes covered were similarly wide, with infectious conditions and their treatment (10.5%), mental health (8.9%), and cancer (8.7%) being the most common.
Projects were predominantly quantitative (99.7%; Table 2) and only 30 projects (4.9%) involved an intervention or experiment. Approximately half the projects (50.1%) consisted of an audit, determined the profile of a group, or determined an incidence or prevalence, and 10.5% investigated one or more aspects of knowledge, attitudes, and practices. Similar percentages of projects used prospective and retrospective data collection, with no marked change over the years. Projects that won the module prize were more likely to have used prospective data collection (15/24; 62.5%). Data were mainly collected regarding patients (61.9%) and in one of the faculty’s training hospitals (primary, secondary, and tertiary healthcare settings, including outpatients and specialist clinics) or laboratories (71.4%). A significant increase in the percentage of projects collecting data about undergraduate students occurred over time: 9.0% in 2002–2008, 11.1% in 2009–2015 and 17.1% in 2016–2022 (p = 0.03). The percentage of projects collecting data about patients declined from 65.3% in 2002–2008 to 55.1% in 2016–2022.
Table 2 Undergraduate medical student research projects’ characteristics and outcomesOnly four projects (0.7%; Table 2) were not completed, i.e. did not go through all the steps of planning, data collection, and reporting. The reasons were as follows: students in the group all failed out of the medical training programme before completion of the research modules (one group), the project was no longer feasible after the supervisor left the country (one group), and the protocol was never finalised to the requirements of the Ethics Committee (two groups).
Approximately one in five projects was published (22.4%). The percentages of published projects increased from 18.8% and 18.3% for projects in the time periods 2002–2008 and 2009–2015, respectively, to 31.8% for projects in the period 2016–2022 (a small number of projects from the latter time period are currently in submission or being prepared for submission). Two projects led to two publications each, resulting in a total of 138 publications, mainly in accredited peer-reviewed journals (n = 137; 99.3%), as full-length manuscripts (n = 123; 89.1%) and with student group members as authors (n = 135; 97.8%). Of the prize-winning projects, 45.8% (11/24) were published. Prospective studies were more likely to be published (78/307; 25.4%) than retrospective studies (57/295; 19.3%). Only two (6.7%) of the 30 studies that involved an experiment were published.
Student FeedbackOf the 155 students involved in projects that were finalised in 2020, 103 (66.4%) responded to one or more of the open-ended questions. Of these, 101 (98.1%) made positive comments and 58 (56.3%) negative comments regarding the research projects. The most common themes are indicated in Table 3. Regarding group work as a negative aspect, some student comments included “participation was sometimes a problem – some members were not fully involved”, “poor communication between group members”, and “group dynamics are always difficult”. However, other students stated a positive experience in this regard, such as “enjoyed working in group!”, “groups made the modules easier”, and “great teamwork and comradery (sic) is learned”. The negative aspect of supervisors related to availability and involvement evoked the following responses: “difficulty getting to meet our study leader – he was very busy; would have appreciated more support from our study leader”, “our study leader wasn’t very involved and didn't always know what was going on in our study”, “the study leader wasn’t available when help or guidance was needed”, “study leaders that are not committed to the project”, “the study leader availability was a problem and cooperation we were quite alone most of the project with module leaders almost giving better guidance”. However, comments such as “the fact that study leaders as well as module heads and members are so involved helped ensure projects are finished on time and that we actually knew what was happening and what we had to do” and “our study leader was also excellent” were also made.
Table 3 Most common themes emanating from students’ open responses regarding research projects—2020 module evaluationForty-eight students (46.6% of those completing the evaluation forms) made some suggestions, mainly regarding organisation/guidelines (11 respondents), supervisors (10 respondents), and module time or timing (9 respondents).
More than 80% (129; 83.2%) of students completing their projects in 2020 responded to at least some of the closed-ended questions. Their responses are summarised in Table 4. More than 70% of responding students indicated that the time was sufficient, that supervisors were available and gave good guidance, and that the modules were informative. Only 59.4% of students agreed that the relevance of the modules to the practice of medicine was clear and 65.9% that the modules were essential in the programme, with approximately 30% of students being unsure.
Table 4 Student responses to closed questions regarding research modules—2020 module evaluation
留言 (0)