A CEH is an uncommon entity described as an organized blood collection that increases in size for more than a month after the initial hemorrhagic event without histological neoplastic features. These are distinct from general soft-tissue hematomas, which form acutely in the presence of bleeding diatheses, anticoagulant therapy, surgery, or trauma, resolve spontaneously, and gradually decrease in size. Pathologically, CEH is characterized by a central mass of blood, a wall of granulation tissue, and dense peripheral fibrous tissue. Its pathogenic mechanism is not fully understood. However, it is assumed to be caused by an inflammatory response inside the cyst. The fibrin matrix and cellular breakdown products of leukocytes, erythrocytes, hemoglobin, and platelets activate the inflammatory process resulting into a well-defined fibrous cavity [2]. These factors increase vascular wall permeability and bleeding from dilated capillaries in the granulation tissue, resulting in the subsequent growth of the hematoma. CEH can develop at any location in the body, such as the subcutaneous tissue and muscles of the arm or legs, brain, and thorax, but rarely in the abdomen. In a review of 204 CEH cases by Syuto et al., only 10 cases located in the abdomen. Among these, only 7 cases were found in the retroperitoneal space, which located around kidney or iliac fossa [3]. In the pleural cavity, respiratory movements and constant coughing can cause the growth of hematomas. In our case, the constant movement of the duodenum and aortic pumping could have caused hematoma growth [4]. Most CEHs start out as very small traumatic hematomas, though, as in the present case, detecting the initial hematoma is difficult, which means suspecting CEH from medical history would be almost impossible.
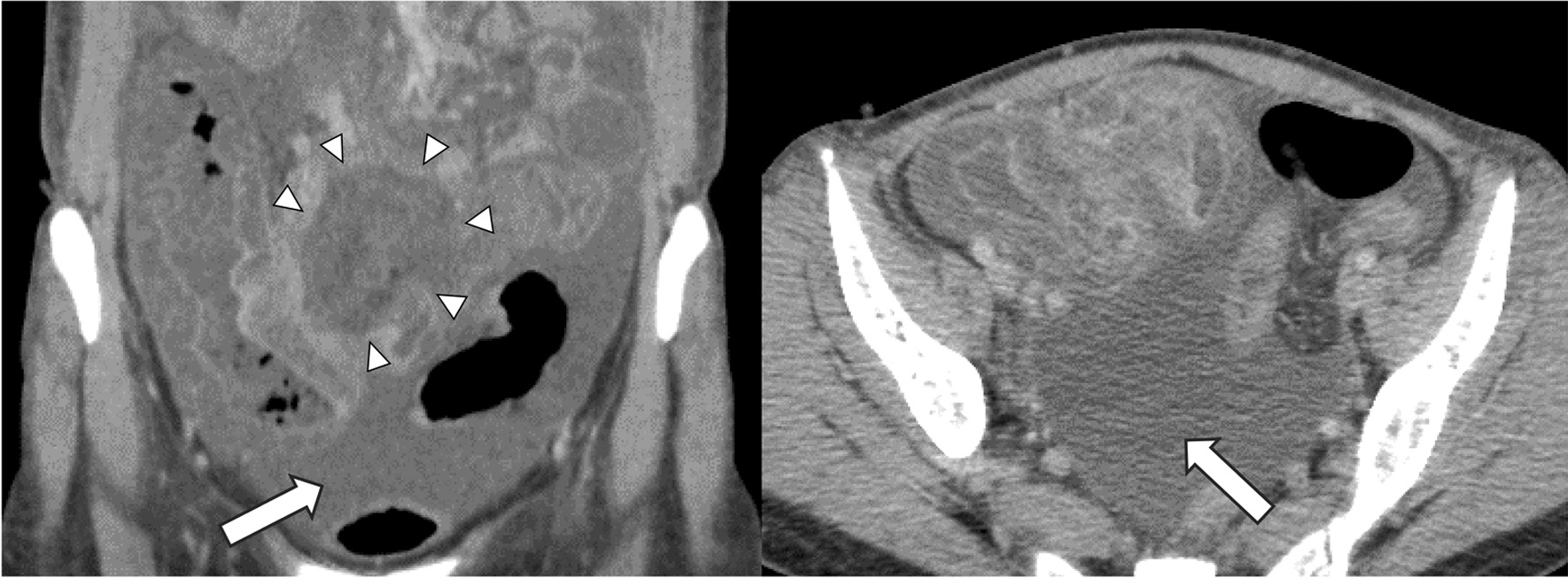
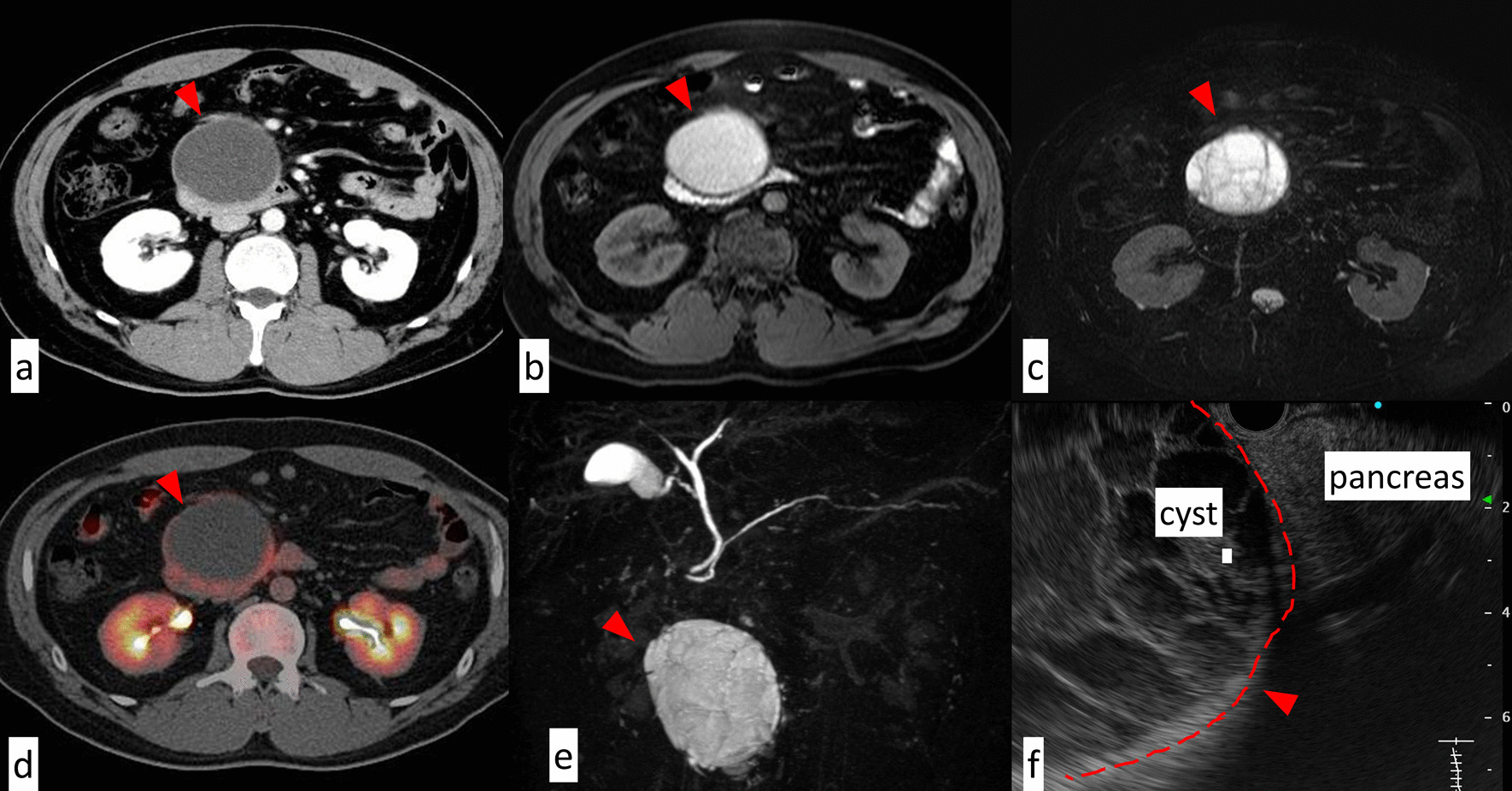
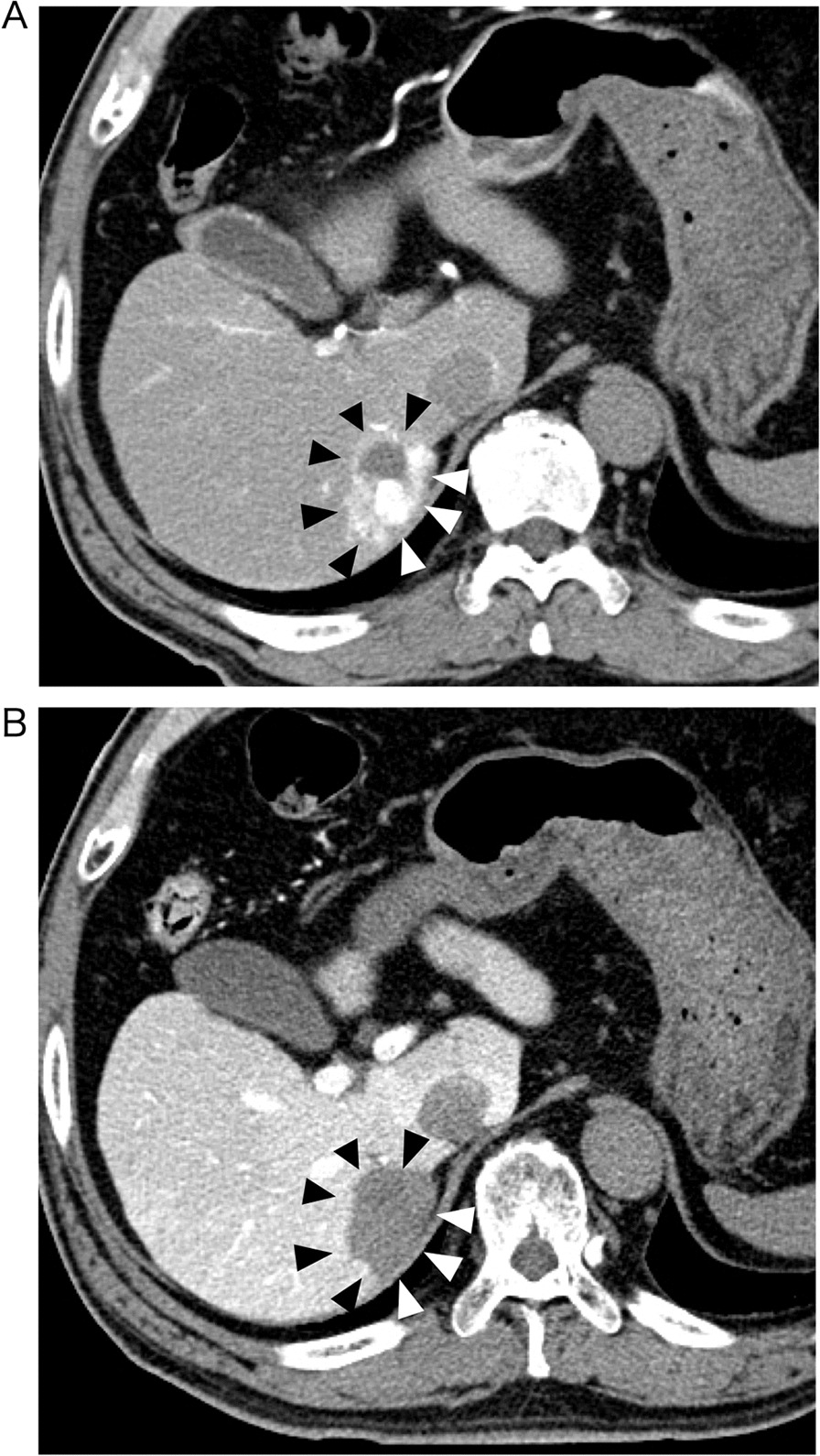
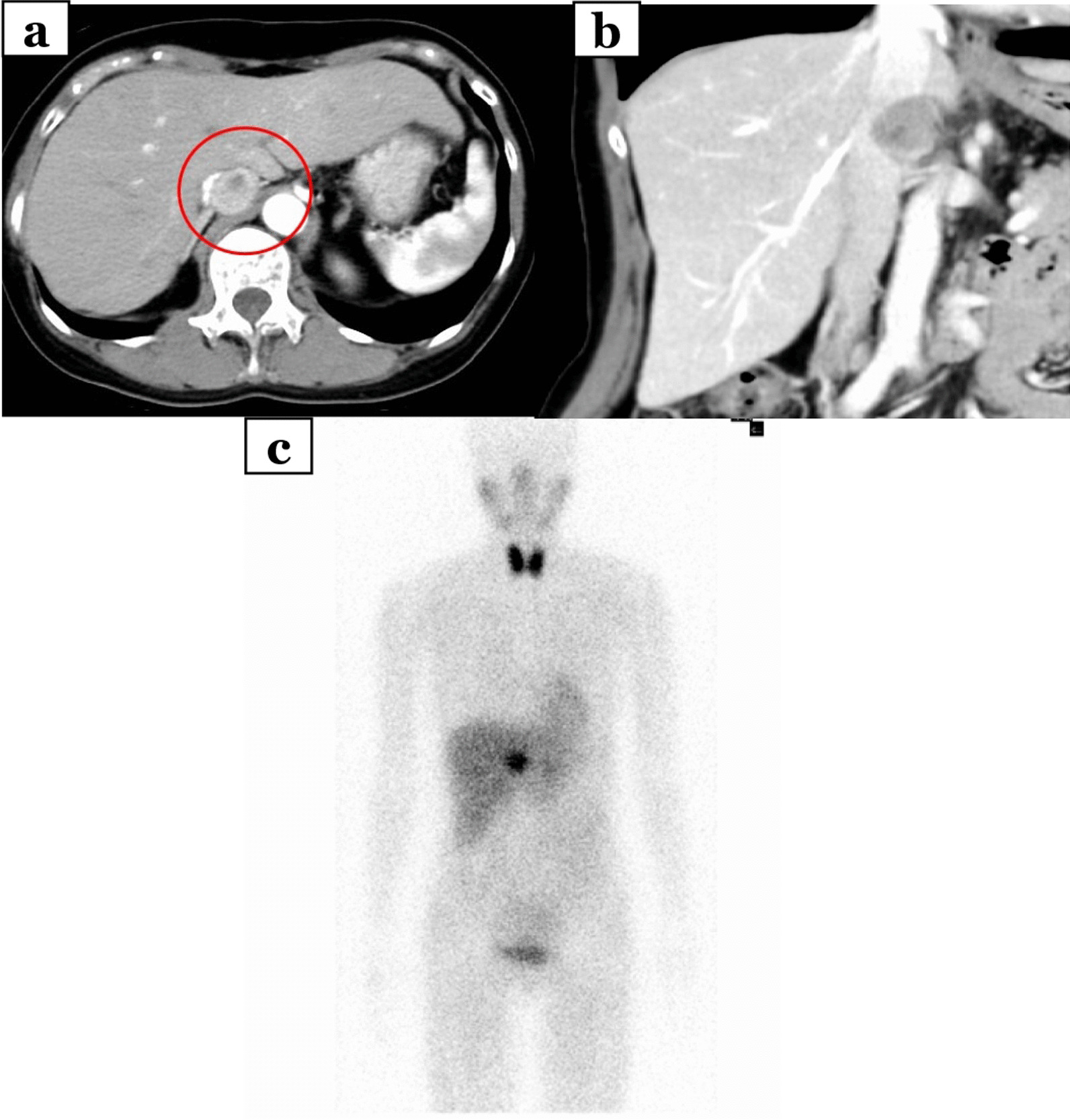
However, the way to diagnose with CEH in image inspections has not been established. CEH often exhibits a mosaic sign in T2-weighted MRI, which represents fresh and old blood, indicating repeated bleeding in the cyst [5], like in this case. This is typical of CEH, although hemorrhage from tumor lesions cannot be completely ruled out. As for PET-CT, the FDG uptake seen only in peripheral rim of the mass, reflecting the inflammatory cell infiltration and granulation tissue in the wall, is said to be characteristic in CEH [6], however, it was not detected in our case. Besides, CEH resembles any tumor depending on the location. In this case, the hematoma located at the pancreatic head and mimicked pancreatic cyst. Searching in PubMed with the keyword of ‘chronic expanding hematoma’ and ‘retroperitoneal’, we found 9 cases of CEH in retroperitoneal space, all of them were Japanese reports. Most of them were located at comparably wide space, such as around kidney or iliopsoas muscle, and none of them contacted pancreas. Hisa et al. reported MCN accompanied by a huge mural organized hematoma with internal capillary vessels and hemorrhaging, which seems to be pathologically and morphologically similar to CEH [7]. So, distinguishing CEH compressing the pancreas from MCN with huge cyst seems to be difficult. In retrospect, the EUS in this case indicated that the cyst was compressing the pancreas without originating from it, which is uncharacteristic of pancreatic cysts. The EUS findings might be useful for estimating the origin of the cystic lesion and it is important for surgical strategy to perform neither too much nor too little resection.
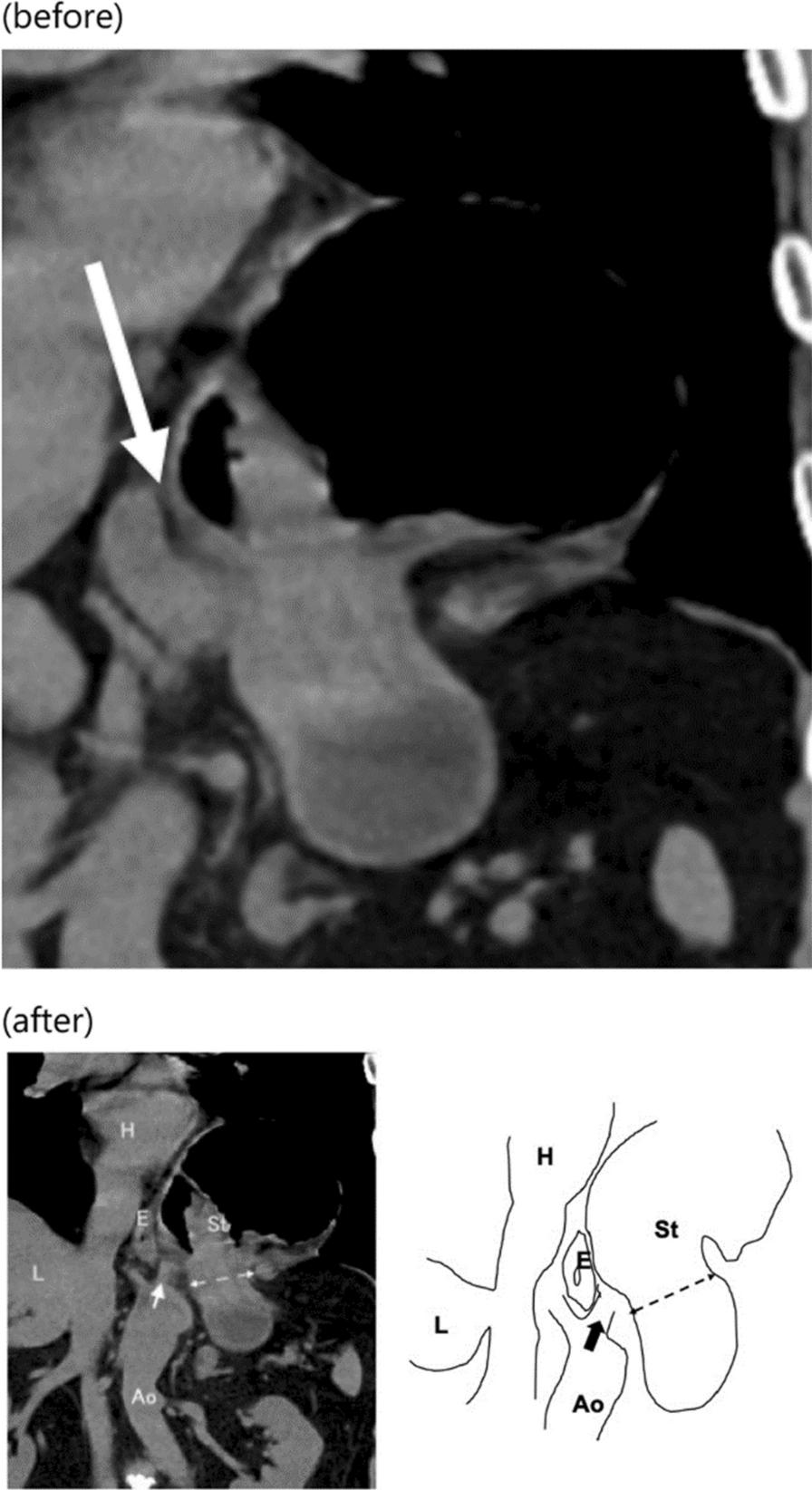
Treatment for CEH involves the complete removal of the fibrous capsule, which is responsible for bleeding inside the hematoma. Recurrence after incomplete resection has been previously reported [8]. Moreover, continuous long-term endothelial stimulation in CEH can contribute to neoplastic transformation. A previous report has noted that angiosarcomas can arise from chronic expanding hematomas at the periphery of the pseudocapsule [9]. Weiss et al. reported that hematomas were associated with approximately 5% of malignant fibrous histiocytomas [10]. Besides, it is impossible to diagnose as hematoma preoperatively and we performed the operation suspecting a benign or premalignant tumor such as SPN or MCN. It means damaging the cyst wall causes the risk of peritoneal dissemination and mucus leakage. Consequently, a complete resection is required. However, it is sometimes difficult because of abundant vascularization, leading to massive bleeding and fibrous adhesions to neighboring organs. There are reports of concurrent resections of the lung [4] or bile duct. Conversely, in some cases, resection of entire pseudocapsule was difficult due to adhesions to the aorta [3] or chest wall [11]. In our case, the cyst was sizeable and adhered to the pancreas and duodenum, however, it didn’t touch them so broadly and had distance with the pancreatic duct, so we decided to perform enucleation, instead of pancreaticoduodenectomy.
In such case, adding a hand-assisted port enabled us to precisely recognize the capsule margins and secure the visual field of the operation through cautious compression of the hematoma, which enables oncologically safe and minimally invasive operation.




留言 (0)