Concept of Michael’s diverticulum
The Meckel’s diverticulum (MD) is a finger-like protrusion on the wall of the distal ileum. It is a congenital malformation that results from incomplete vitelline duct degeneration. MD is the most common congenital abnormality of the gastrointestinal tract [1]. Its incidence is 2 to 4%. MD is a true diverticulum that contains all the layers of the intestinal wall [2]. The location of the MD is uncertain, but it is usually found within 100 cm of the ileocecal valve [2]. The classic diagnostic criteria for MD are as follows: the diverticulum has to be located on the antimesenteric border, within 2 ft proximal to the ileocecal valve, contains all five layers of the small intestine, and has its own blood supply [3]. In the present case, pathology confirmed that we were facing a true diverticulum with all layers of the intestinal wall. The 3.5 cm long and 3 cm wide diverticulum was located on the distal ileum 30 cm from the ileocecal valve.
Meckel’s diverticulum and its complications
MD is asymptomatic in most affected individuals, with a 4.2–16.9% probability of symptomatic presentation [4]. The clinical presentation ranges from intestinal obstruction to bleeding, inflammation, and perforation [5]. While children with MD more often present with gastrointestinal bleeding, intestinal obstruction is the most common presentation in adults. Perforation of the MD is extremely rare [5]. Most often when fecaliths obstruct the diverticulum, leading to inflammation and necrosis. More rarely, perforation is due to foreign body perforation. Foreign bodies, including fish bones, gallstones, enteroliths, marbles, bullets, and phytobezoars, have been reported in less than 2% of symptomatic MD. The foreign bodies that cause perforation of MD are more often sharp objects, such as fishbones and date pits [6]. In this case, the patient accidentally ingested dentures, which perforated MD, resulting in an abdominal abscess. This unexpected complication eventually led to intestinal obstruction. Edentulous individuals are also at a higher risk of ingesting foreign bodies, including dentures, owing to reduced sensation in the oral mucosa and poor motor control of the laryngopharynx [7]. Another important issue that increases the risk of denture ingestion is the lack of patient awareness regarding the need for regular check-ups and denture changes or compliance [8]. It is worth mentioning that fixed dentures, as well as removable dentures, can be accidentally ingested. Therefore, patients wearing dentures should be advised to regularly review their condition, and patients with loose dentures should see a dentist as soon as possible.
Imaging diagnosis of Meckel’s diverticulum
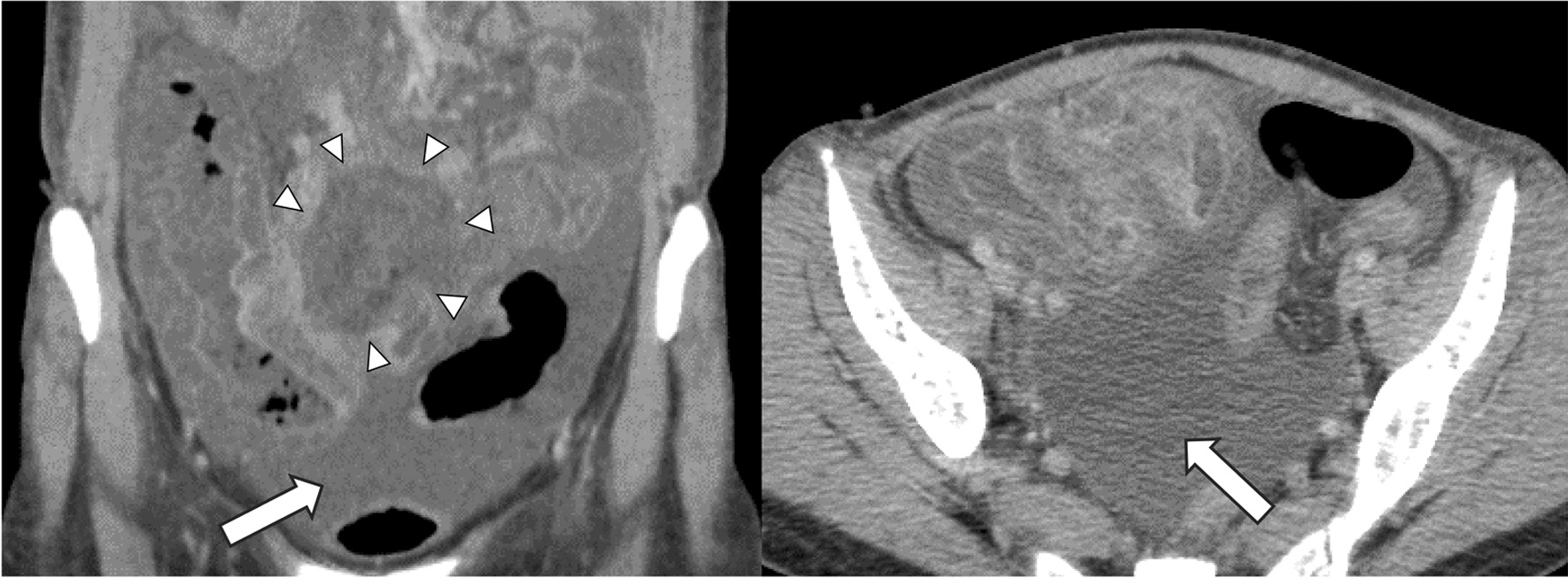
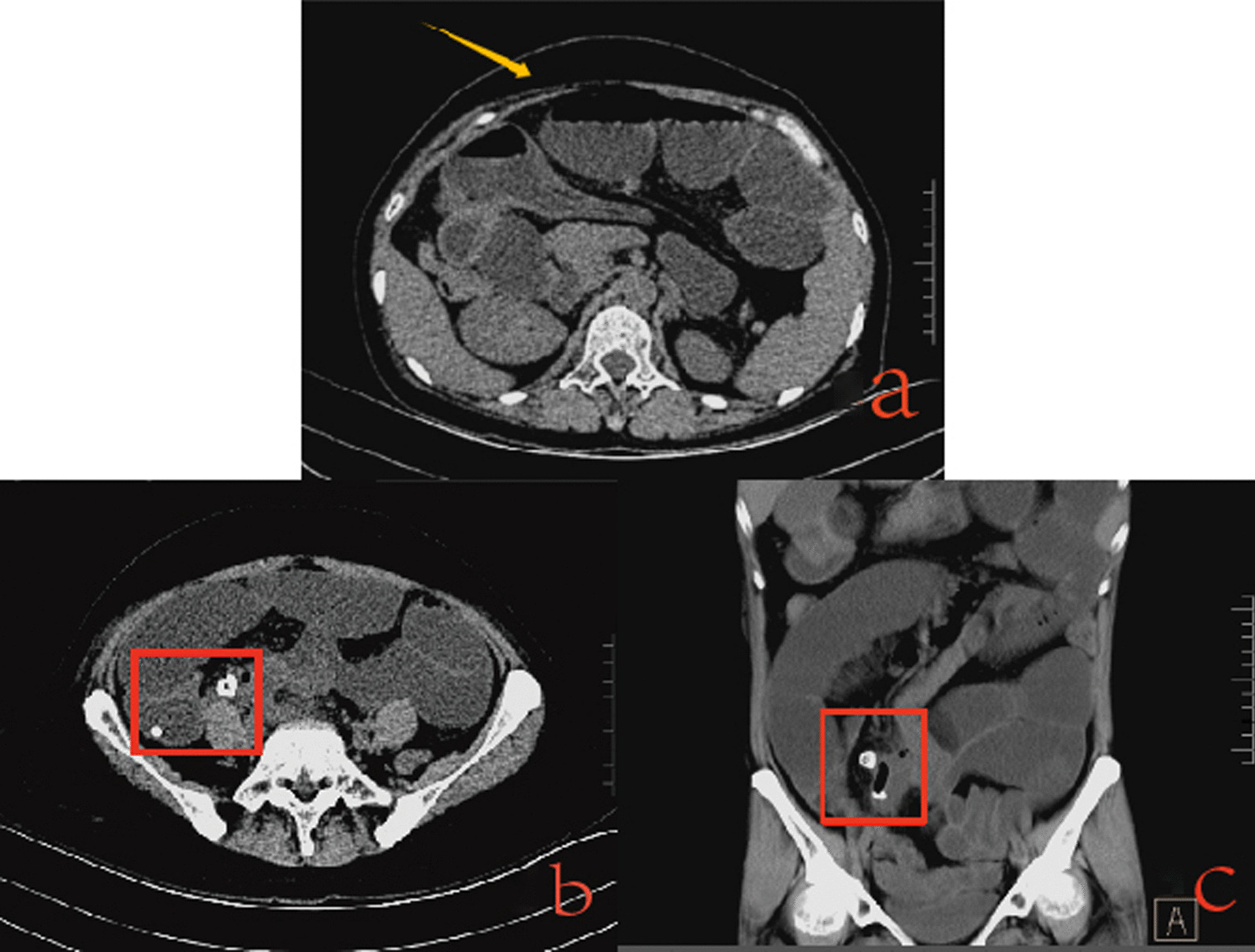
Imaging has limited value in the diagnosis of MD. Only 10% of symptomatic MD are definitively diagnosed preoperatively [5]. Acute appendicitis is the most common cause of misdiagnoses. Plain X-ray, barium studies, and computed tomography (CT) scans are seldom beneficial for the preoperative diagnosis of diverticulum. They can be normal or show nonspecific changes [5]. It is often difficult to make an accurate judgment before surgery, and clinicians must assess it in conjunction with the patient's medical history and clinical symptoms. As in the present case, the diagnosis was only made intraoperatively. Although the diagnosis of MD has posed challenges for surgeons, new diagnostic methods, such as capsule endoscopy, double-balloon enteroscopy, and 99mTc pertechnetate scintigraphy, have emerged in recent years [9, 10]. With further verification of the feasibility of these tests, the diagnosis of MD has greatly developed.
Treatment of Meckel’s diverticulum
It is generally accepted that resection is the treatment for symptomatic MD. Although exploratory laparotomy has traditionally been the standard approach, it has been shown that laparoscopic approaches have equivalent outcomes and may reduce the overall length of stay [11]. In a study based on the analysis of the NSQIP Pediatric database comparing laparoscopic, laparoscopic converted to open, and open resection in 681 pediatric cases, Skertich et al. demonstrated low rates of postoperative complications and few significant differences between laparoscopic and open surgery. The most common complications observed were surgical site infections, bleeding, and readmission. In addition, the conversion rate from laparoscopic to open surgery was high (27%) [12]. Therefore, when dealing with acute abdomen caused by foreign bodies that require surgical treatment, surgeons should choose between laparotomy or laparoscopic surgery, according to the specific circumstances. In this case, the swelling of the small intestine and adhesion of the pelvic cavity led to a final change in the surgical plan.
When selecting between diverticulectomy or segmental bowel resection with re-anastomosis for resection of MD, it should be based on the morphology of the diverticulum and the condition of the surrounding ileum. Generally, simple diverticulectomy is recommended as long as the base of the diverticulum is small relative to the ileum and there is no inflammation or perforation at the base [13]. Segmental resection of the ileum containing MD is recommended if the base is broad or if diverticulectomy results in significant luminal narrowing. Ileal resection is also recommended if the base is inflamed, perforated, or has a bleeding ulcer [14]. Brungardt et al. analyzed 506 adult cases in the NSQIP database comparing diverticulectomy with segmental resection and found similar rates of complications and mortality within 30 days. Additionally, the most common complications in both groups were readmission, sepsis, wound infection, and reoperation [15]. In the present case, we decided to perform diverticulectomy and partial ileectomy because ischemia and perforation of the local diverticulum wall occurred, part of the ileal adhesions were angulated, and blood circulation in the bowel was poor.




留言 (0)