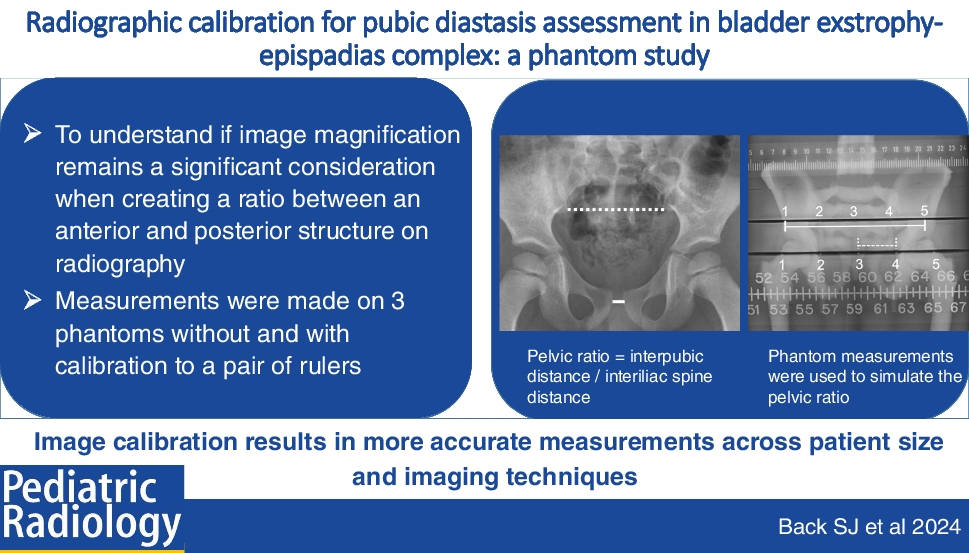
Pubic bone diastasis in patients with ECC correlates with significant differences in the pelvic floor musculature. The osseous relationships change over the course of surgical reconstruction and long-term follow-up [3]. While not previously demonstrated in the literature, to our knowledge, we postulate that a wider or narrower diastasis is associated with more or less severe pelvic floor deformity which may portend the risk of complications and influence both short- and long-term outcomes. As radiography is a mainstay imaging application for patients with ECC, understanding the osseous anatomy and potentially quantifying these relationships prior to and during reconstruction may help further guide treatment. Moreover, pubic diastasis after various osteotomies and traction methods has been associated with outcomes, which led to the use of the degree of diastasis as a measure of how well the osteotomy or traction worked [11, 12]. However, these studies do not describe calibration or an internal ratio to standardize the measurements, and as such, these measurements may not be an accurate depiction of what is occurring with the bones. We designed this phantom study using different exam techniques and body sizes to simulate the radiographic measurement of pubic diastasis; the linear distance between the posterior inferior iliac spines; and the creation of a ratio between these values to understand the differences between uncalibrated and calibrated measurements. To determine if radiographic measurements can be compared to one another over the growth and development of a child, we considered several questions. First, can measurements from different radiographic equipment and techniques (thoracoabdominal image of a neonate, abdomen or dedicated pelvic radiographs) can be compared to one another? In particular, we wanted to know if the portable radiographic units used to obtain images in the neonatal intensive care unit and operating room are comparable to the fixed units used for outpatient imaging follow-up. Second, can calibration mitigate the effects of magnification when making measurements on radiographs? As an anterior structure, the measurement of pubic diastasis is subject to greater magnification than measurements of posterior anatomy. Magnification is increased during growth and development as the distance between the pubis and the radiographic image detector becomes greater with increased pelvic girth. Lastly, can creating a ratio using an internal measurement standardize and account for these variables?
In this phantom study with excellent interrater agreement, we found statistically significant differences in the absolute measures with the use of calibration. Calibrated measurements were shorter than uncalibrated ones and closer to the true distance.
Here, calibration also helped to correct this projection magnification associated with the pubis being an anterior structure with greater object to image distance than for the posterior inferior iliac spines (Fig. 5). The differences between calibrated versus uncalibrated measurements increased as the anteroposterior diameter of the phantom (child) increased with age and were also corrected with calibration, and were as high as 12.5 mm difference in anterior measures. Uncalibrated measurements of the abdomen and pelvic radiographic techniques were similar, whereas there were differences between uncalibrated measures of these techniques compared to the thoracoabdominal technique. However, with calibration, there was no difference between any of these techniques. These observations support the use of calibration when comparing measurements obtained via different radiographic techniques and on differing sized children.
Here, we standardized the source to image distance for the installed and portable radiography units. However, the portable unit has an inherently smaller object to image distance, as the phantom (child) is positioned on top of the detector while the departmental units have an additional 2 inches between the anatomy and the image. Calibration made measurements obtained from different equipment more uniform.
Normative reports of pubic distance were done by assessing abdominal or pelvic radiographs in 888 children aged 0 to 16 years, where no difference was found in pubic distance between genders or radiographic techniques when comparing measures of patients who underwent both studies [13]. Without considering projection magnification, the inter-pubic distance was greatest in infants but remained below 1 cm throughout childhood with a relatively consistent distance from 4 to 16 years of age [13]. McAlister et al. assessed pubic distance to establish a normative range in children in order to recognize diastasis, with a suggested maximal diameter of 0.84 mm using an electronically calibrated measuring tool [14]. While the authors concur that there is no significant difference between male and female children, one group did not account for the effects of image magnification and the other used the electronically calibrated measuring tool of the imaging system. The necessity of calibration depends on the acceptable measurement error for a given application.
Radiography is a common imaging modality in both pre- and postoperative assessment in fields like orthopedics and dentistry. Magnification has been a significant concern in the preoperative measurements made for templating prosthetic size for adult total hip arthroplasty and in the postoperative evaluation of prosthetic subsidence because small distances (2–4 mm) are clinically significant [15]. In a cohort of patients who underwent orthopedic fixation for trauma, there was magnification of the implanted hardware, between 13 and 29% compared with the known size, which was greatest in central anatomy (proximal femur) [16]. In a study of a length standard phantom for dental radiographs, the authors report a deviation in the linear length of −3.37 ± 0.15 mm without calibration and improvement to −0.11 ± 0.10 with image calibration [17].
One approach to standardize measurements for comparison between patients has been to create a ratio between the desired measurement and a common denominator. This was applied to the assessment of ulnar variance in a group of adult patients with distal radial fractures. Ulnar variance was divided by the capitate height which served as an internal control for images that were uncalibrated or unscaled [18]. However, if magnification and variables that may affect magnification (body size, exam technique, radiographic equipment) have significant effect on the ratio, then a standardized and calibrated approach is necessary to assess such measurements for use in clinical care.
There are limitations to our study. As a phantom design, measurements of clinical radiographs will be needed to confirm these observations. When placing a standard or calibration ruler, it is ideal for this object to be at the same level as the anatomy that is being measured. While we have positioned two separate rulers in this study, our positioning does not account for soft tissue thickness, which would limit the ruler position relative to the bone anatomy. Many orthopedic practices utilize a height-adjustable spherical fiducial marker for calibration of pelvis and leg-length radiographs. Unlike a ruler placed atop a patients’ thighs, such a device is not subject to angular deflection and can be placed at the palpated level of the pubic symphysis [19]. We utilized radiographic vendors in our institution and while we think these principles will hold for other vendors, we cannot be certain.
We have confirmed that anterior structures have greater magnification on projection imaging than posterior structures. Based on this magnification difference, the outcome of the pelvic ratios without and with calibration are expected. With the increased numerator on the uncalibrated images, the ratio should be larger when measurements are uncalibrated versus calibrated. However, the pelvic ratios decreased from approximately 0.26 to 0.27 on uncalibrated images to approximately 0.23 to 0.24 when calibrated, a difference of only 0.04. The role of the pelvic ratio as an imaging marker for surgical outcomes is an area of active research. This small numerical difference in the ratio, while statistically significant in this study, may not be clinically relevant. However, if distances are measured on clinical radiographs, we believe it is best to obtain the most accurate measurements, which require calibration. This may be particularly important for research comparing outcomes from different surgical groups with potentially varied imaging techniques and for groups comparing measured pubic diastasis rather than pelvic ratios.







留言 (0)