
記住我






This prospective, institutional review board (IRB)-approved, single-site study included 50 pediatric patients undergoing routine, non-contrast clinical brain MRI examinations enrolled between July 2022 and January 2023. Exclusion criteria included age less than 2 years, need for imaging under general anesthesia or sedation, and history of neurologic surgery and/or the presence of intracranial implants. Informed consent was obtained from all participants, and informed assent was obtained, as appropriate.
All imaging was performed on a single 1.5-Telsa MR scanner (Ingenia; Philips Healthcare; Best, the Netherlands) using the body coil transmit and a 15-channel receive only head coil. Clinical 2D T2-weighted (T2W) FLAIR (repetition time (TR)=11,000 ms, inversion time (TI)=2,800 ms, echo time (TE)=140 ms, acquired in plane resolution=0.79 mm×0.78 mm, 4-mm contiguous interleaved slices; compressed SENSE (CS) acceleration factor=1.6) images from our clinical imaging protocol were reconstructed with both standard CS (medium denoising) image reconstruction and AI “strong” denoising (selected from a 4-point scale provided by vendor: weak, medium, strong, and maximum) algorithm (SmartSpeed; Philips Healthcare, Best, The Netherlands). All T2W FLAIR images (Figs. 1, 2, and 3) were reviewed independently in a dedicated research picture archiving and communication system (PACS) by two study neuroradiologists, both with added qualifications in neuroradiology and one with additional added qualifications in pediatric radiology. The research PACS system used (Merge Healthcare, Version 8.1.6.7) allowed the radiologists to be blinded to patient information and clinical data during the review process; however, the radiologist was not blinded to image reconstruction method during side-by-side review. AI images were evaluated on a 3-point scale (poor, sufficient, excellent) for overall image quality, subjective assessment of signal to noise ratio (SNR), various artifacts, and diagnostic preference. Each sequence was also rated on a 3-point scale to indicate whether AI increased, decreased, or had no effect on image quality compared to the standard reconstruction. Additional imaging features were assessed and compared between the AI and standard reconstruction images and included CSF artifacts, motion artifacts, susceptibility artifacts, gray-white matter differentiation, image sharpness, flow void visualization, and extracranial structure evaluation (Supplementary Material 1). The presence of pathology, normal variants, or lack thereof were also commented on.
Fig. 1
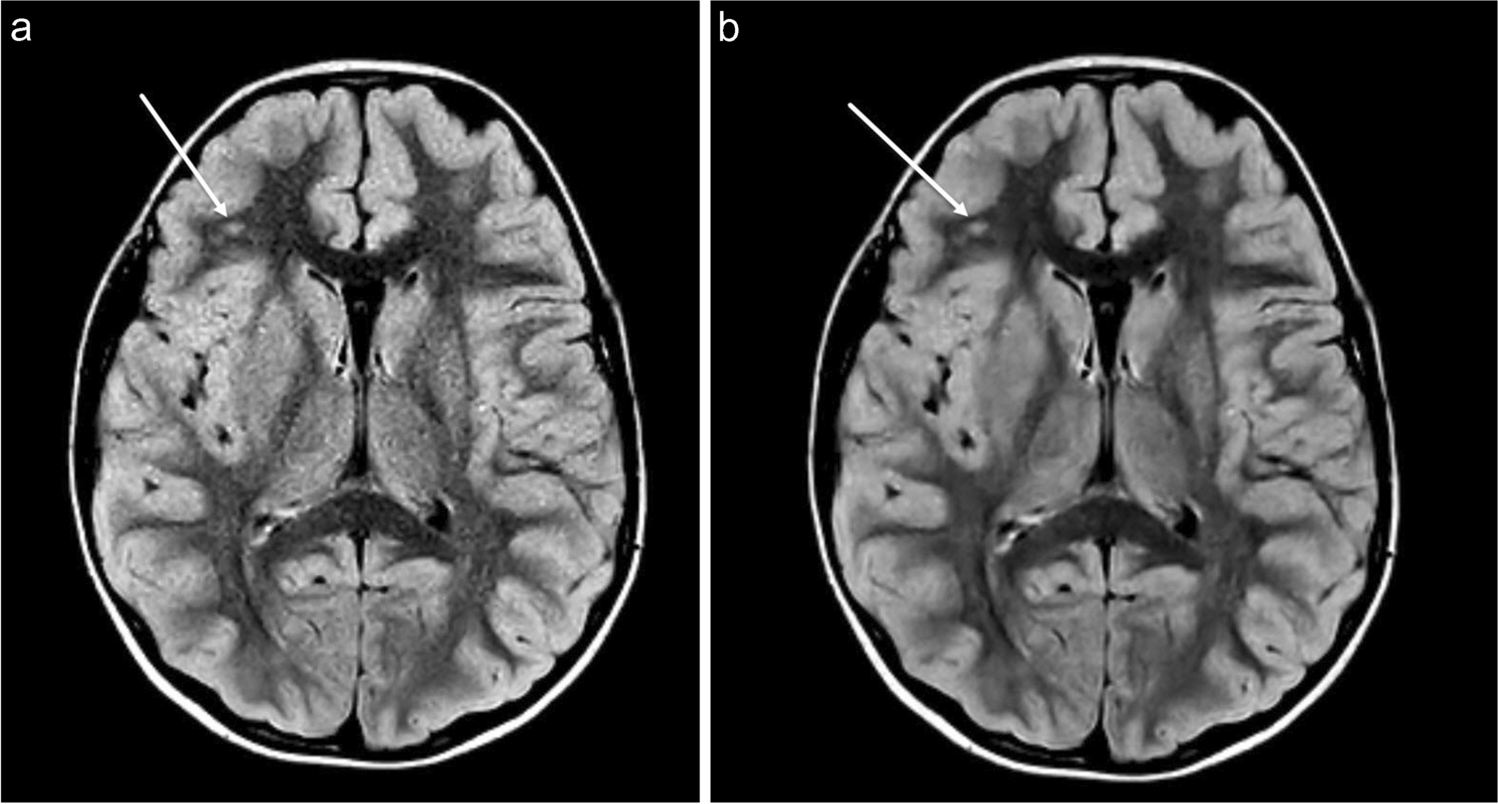
a-b Axial T2W FLAIR CS=1.6 brain MR images in an 8-year-old female presenting with repeated episodes of vomiting in the middle of the night without (a) and with (b) AI image reconstruction (SmartSpeed; Philips Healthcare). The AI image shows a reduction in image noise compared to the standard image reconstruction. There is also a focus of T2W FLAIR hyperintense signal in the right frontal white matter (arrows), doubtful clinical significance however is clearly reproduced on the AI reformat. Note is also made of a cavum septum pellucidum, normal anatomic variant, also accurately reproduced
Fig. 2
a-b Axial FLAIR CS=1.6 brain MR in a 14-year-old female presenting with new onset of headaches and dizziness without (a) and with (b) AI image reconstruction demonstrates global reduction in image noise and ill-defined signal abnormality in the right thalamus (arrows) suspicious for infiltrative neoplasm, reproduced on AI reconstruction
Fig. 3
a-b Axial T2W FLAIR CS=1.6 brain MR in a 8-year-old male with known diagnosis of tuberous sclerosis with standard (a) and AI (b) reconstruction demonstrating a dysplastic lesion in the right parietotemporal junction involving the subcortical and transmantle white matter (solid white arrows). There are additional smaller T2W FLAIR hyperintense foci in the bilateral periventricular white matter (dashed arrows), also accurately reproduced on AI reconstruction
Quantitative analysis was performed using Philips IntelliSpace Portal (Version 10.1, Philips Healthcare). Regions of interest (ROIs) were manually placed by one neuroradiologist in the right putamen and right frontal white matter, and the mean and standard deviation of the signal within each ROI were used to calculate apparent signal to noise ratio (aSNR) gray matter, aSNR white matter, and apparent gray-white matter contrast to noise ratio (aCNR) (Fig. 4). aSNR was calculated using the following equation: aSNR tissue=µ tissue/σ tissue. aCNR was calculated using the following equation: aCNR white matter–gray matter=|(µ white matter−µ gray matter)/√? white matter 2+? gray matter2| (µ, signal intensity; σ, standard deviation) [3].
Fig. 4
a-b Axial T2W FLAIR brain MR images in an 11-year-old male demonstrating circular ROIs placed in the right frontal white matter and right putamen for signal analysis in the standard reconstruction (a) and AI reconstruction (b) images
Statistical analysis was performed using Excel (2021, Microsoft) spreadsheet mathematic functions including mean values, standard deviations, value count, and t test results. P-values less than 0.05 were considered statistically significant. Descriptive statistical analyses of the independent reviews were performed. We did not use kappa coefficients due to unbalanced observation across scores.
留言 (0)