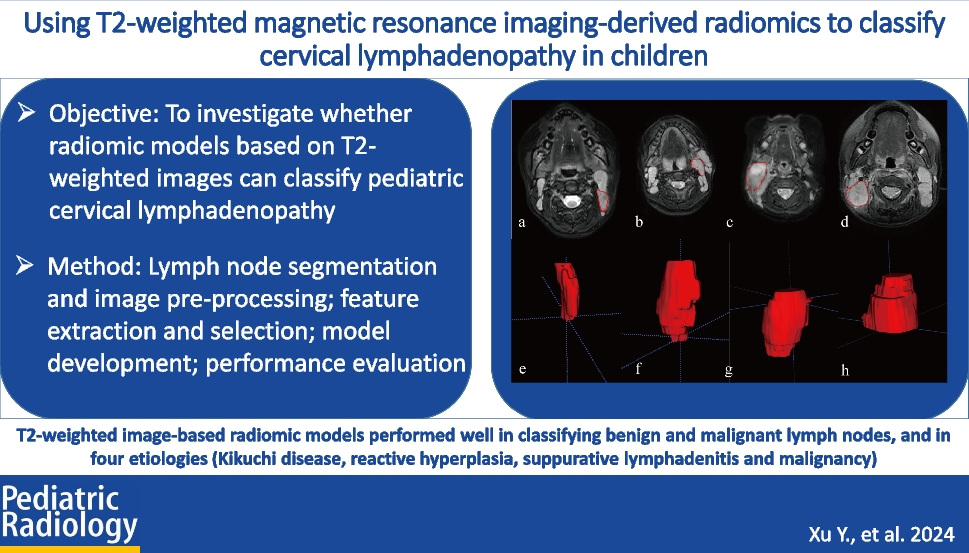
In this proof-of-concept study, we explored the feasibility of distinguishing pediatric cervical lymphadenopathy based on MR images. Two radiomics models were developed. Good performance was shown not only in distinguishing malignant from benign lymph nodes (an AUC of 0.80 in the testing set), but also in distinguishing four different types of lymph nodes (an AUC of 0.96, 0.80, 0.82, and 0.82 in the testing set, respectively). In particular, our model demonstrated a significant advantage on identifying Kikuchi disease. This might be a promising non-invasive tool to assist the evaluation of cervical lymphadenopathy.
In routine clinical practice, radiologists use semantic characteristics to distinguish pathologic from benign lymph nodes: size, shape, borders, clustering, and internal heterogeneity. Information provided is still limited and may be influenced by the observer’s naked eyes. Radiomics, a high-throughput approach that extracts quantitative features from images and transforms them into mineable data [17], is independent of the observer’s experience and can extract more subtle characteristics. Traditionally, size and shape are the most common criteria, a larger and rounder lymph node tends to be abnormal; however, this may not be applicable to children as their lymph nodes undergo physiological hyperplasia. In a recent study of normal children, identifiable lymph nodes in the head and neck were calculated and a mean of the short axis greater than 10 mm was reported [18]. Therefore, it may be more reliable to judge by shape. However, the present measurement of shape is determined by a ratio of short and long axes; the result may vary with planes. In our study, the feature original shape sphericity was an important feature to classify benign and malignant lymph nodes. By measuring lymph nodes in 3-D, we were able to have a comprehensive understanding from the overall perspective rather than a single maximum section.
In addition, the feature LoG-sigma-5.0mm_3-D_GLCM_IMC1 had the highest impact on classification of benign and malignant lymph nodes and Original_GLCM_IMC1 had the highest impact when classify Kikuchi disease from the other three cervical lymphadenopathies. This is a reasonable finding as texture features have been known to measure internal heterogeneity and explain the spatial interdependence or co-occurrence of information between adjacent voxels [19]. GLCM is used to describe the joint distribution of two neighboring pixel gray scales with spatial location relationship. Informational measure of correlation (IMC)1 is one of the GLCM features that quantify the complexity of the texture. Generally, greater complexity in heterogeneity implies a greater likelihood of malignancy, but for Kikuchi disease, whose characteristic is varying degrees of necrosis with abundant karyorrhectic debris in paracortical areas, such intranodal necrosis is microscopic that often is not apparent enough to be recognized by radiologists. In a CT characteristic analysis, nodal necrosis was reported in only 16.7% of patients with Kikuchi disease [20]; in another MRI finding, necrosis which was shown in a hypointense manner on T2-weighted images was found in less than half Kikuchi disease patients [21].
Our results partially confirm the difficulty of visual identification by radiologists for most of the selected features belonging to high-order features. There is evidence that preprocessing filters can further decouple texture features [22]. By changing the ratio of signal frequency, wavelet filters may reduce noise and achieve compact feature representation [23]; LoG filter acts as an edge enhancement tool to emphasize areas of gray-level changes, where a higher sigma value represents coarser textures, in other words, gray-level changes over a larger distance [24]. Our findings reveal the subtle distinctions between lymph nodes that can only be distinguished by de-noising and enhancing filters. Our model may help to compensate for the inadequacy of traditional reading.
Previous studies mainly focused on US images. Liu et al. developed a multi-class US-based radiomics model to classify tuberculous, lymphomatous, and reactive and metastatic lymph nodes with an AUC of 0.673, 0.623, 0.655, and 0.708 for each disease [25], respectively, and Zhu et al. built a hierarchical diagnosis model via a deep residual network algorithm based on dual-modality US images (B-mode US and color Doppler flow imaging) [26]. There are also studies that demonstrate the utility of a CT-based radiomics classifier [27,28,29]. However, in most studies, only one representative image was chosen and single-section regions of interest for each patient were segmented which resembles core needle biopsy that may not allow for a comprehensive profile of the entire lymph node. The strength of our study is VOIs were manually drawn slice-by-slice of the entire lymph node’s boundary which carry more textural information. Therefore, we have a significant advantage in identifying Kikuchi disease which has variable degrees of necrosis inside lymph nodes.
The study has a few limitations. First, the retrospective nature may introduce selection bias. Second, VOIs were obtained manually, and might have introduced some inaccuracy. Enlarged lymph nodes due to suppurative lymphadenitis were difficult to segment due to extensive diffusion on images, resulting in suboptimal accuracy in the testing set. However, the prominent clinical signs of suppurative lymphadenitis such as raised temperatures can make up for its shortcomings. Third, the lack of an independent testing cohort raises a concern regarding potential generalizability of the proposed model; thus, further validation with a large sample, multi-center, and prospective study is needed. With accumulation of images, further study is expected to develop a computer-aided diagnostic software tool for the detection of small radiographic abnormalities in the neck, with the potential to enhance tissue-based detection.







留言 (0)