Study design
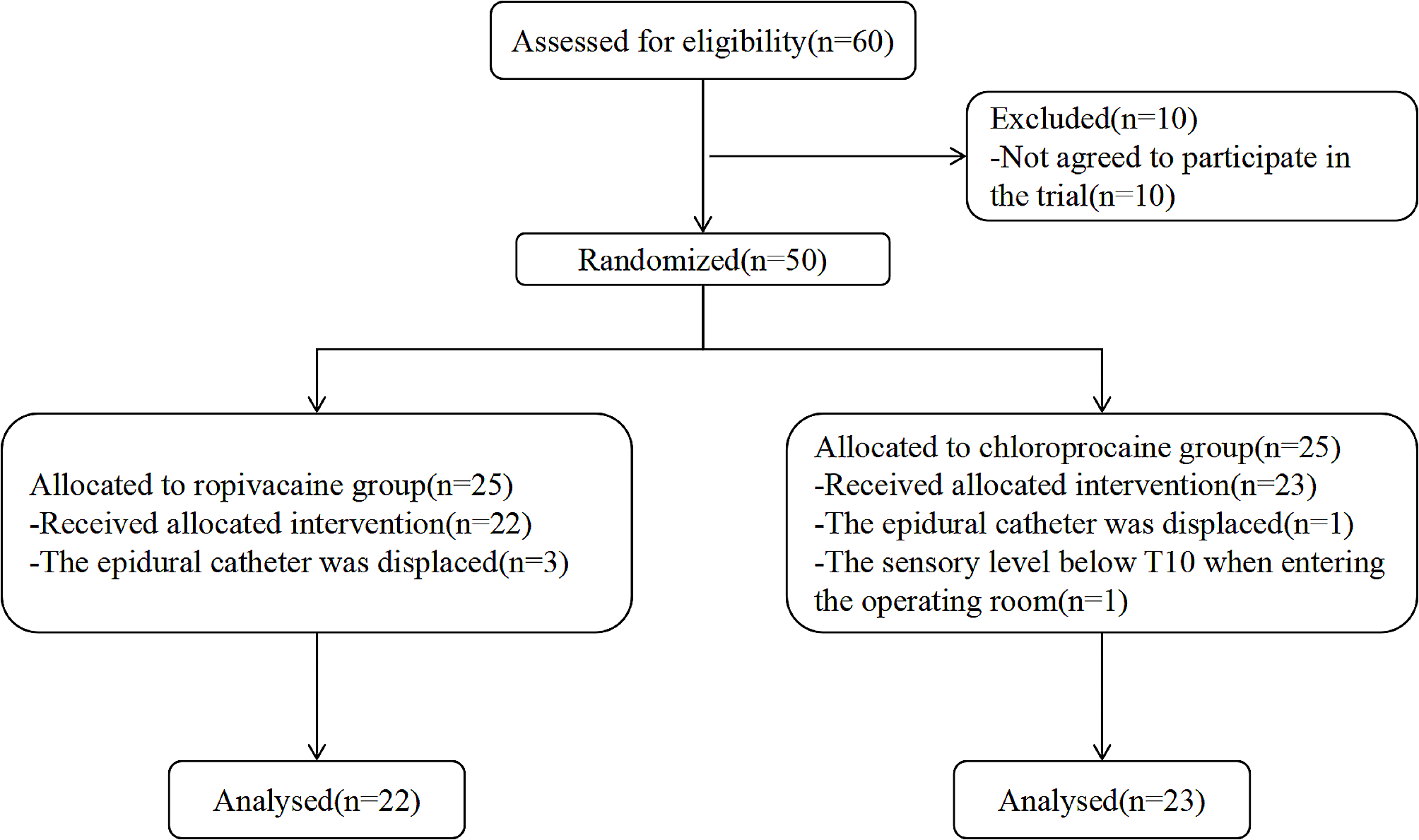
This was a single-center, double-blind, randomized, controlled study that was conducted from November 1, 2022, to April 30, 2023, and approved by The Ethics Committee of Hangzhou Women’s Hospital on September 15, 2022 (IRB: 2022-K(9)-07). Forty-five pregnant women who underwent urgent cesarean delivery while under labor analgesia were selected and randomized in a 1:1 ratio to the 0.75% ropivacaine (RP group) or 3% chloroprocaine (CP group) after providing written informed consent. Inclusion criteria were: (1) being 18 years or older; (2) having an ASA physical status of 1 or 2; (3) being over 36 weeks of gestation; (4) having a singleton pregnancy; (5) having effective labor analgesia (defined as requiring two or fewer intrapartum epidural supplements of 0.2% ropivacaine); and (6) requiring urgent cesarean delivery (category 2 or 3).
Exclusion criteria were: (1) receiving epidural supplementation less than two hours before cesarean delivery or intramuscular pethidine within four hours; (2) requiring emergency cesarean delivery (category 1); (3) having severe fetal anomalies; (4) having pre-eclampsia⁄eclampsia, antepartum hemorrhage, or any form of cardiac disease; (5) being shorter than 152 cm or weighing more than 115 kg; (6) having an allergy to any study drug; or (7) having entered the operating room with a sensory level below T10.
Proposed classification for urgency of caesarean Sect. [16]: (1)emergency: immediate threat to life of woman or fetus; (2)urgent: maternal or fetal compromise which is not immediately life-threatening; (3)scheduled: needing early delivery but no maternal or fetal compromise; (4)elective: at a time to suit the woman and maternity team.
Randomization and blinding
An independent researcher randomized the postpartum women into the 0.75% ropivacaine group and 3% chloroprocaine group in a 1:1 ratio using numbered sealed envelopes. An independent investigator prepared the injected local anesthetic of 0.75% ropivacaine or 3% chloroprocaine. The independent attending anesthesiologist who administered the local anesthetic drug was not involved in other parts of the study and was unaware of the study drug. An independent anesthesiologist who was not informed of the outcome of the group assignment collected the data. Additionally, the group assignments for the included patients, surgeons, and data analysts were concealed.
Epidural labor analgesia
Pregnant women were admitted to the operating room where a constant infusion of lactated Ringer’s solution was administered through an intravenous line. All pregnant women underwent epidural block in the L2-L3 position in the right lateral recumbent position. We used a 17-g Tuohy needle to identify the epidural gap by anatomical landmarks and palpation, which was identified by loss of resistantance to the saline technique. After insertion of the epidural catheter, 3 ml of lidocaine 1.5% was injected by the anesthesiologist. If no sign of spinal block was seen after 5 min, 10 ml of local anesthetic solution (0.1% ropivacaine + 2ug/ml fentanyl) was injected for labor analgesia. If a suitable sensory level was not attained within 15 min of the loading dose, further 5-mL aliquots were given every 10 min for the following 20 min, up to a maximum dose of 20 mL. Subsequently, the first dose was administered through a Programmed intermittent epidural anesthetic bolus (PIEB) pump (ZZB-IV; Nanjing Apon Co., Ltd., Nanjing, China) at 60 min after the end of the loading dose. All subsequent PIEB dosing intervals were fixed at 8 ml/h, with Patient-Controlled Epidural Analgesia (PCEA) set at 8 mL/dose, a lockout time of 15 min and a maximum dose of 35 mL per hour, to establish bilateral sensory levels in the T10 block [6]. Subsequently, if analgesia was inadequate, 10 ml of 0.2% ropivacaine was administered.
Extended epidural anesthesia
If an emergency cesarean section was necessary, the level of pre-existing block to cold sensation was assessed, and motor block was recorded using a modified Bromage score before the pregnant women were admitted to the operating room [17]. The modified Bromage score was as follows: (0) no motor block, able to lift extended leg and flex the knee and ankle; (1) inability to raise extended leg, able to move knees and feet; (2) unable to flex knee; and (3) unable to move lower limb.
An independent attending anesthesiologist administered a test dose of 5 ml of the study drug after confirming negative epidural catheter aspiration and monitored the patient for any indications of an unintentional intrathecal injection. The remaining 15 ml of study drug (0.75% ropivacaine or 3% chlorprocaine) was injected over 3 min. Arterial pressure and heart rate were measured every three minutes.
One investigator marked bilateral T4 levels in the midclavicular line using bilateral nipples as a body surface marker to reduce the previously reported inter-observational differences [18,19,20]. Cold sensory level was measured at 1-minute intervals with 70% ethanol application. The onset of anesthesia (time from the end of the starting dose to the loss of cold sensation bilaterally to T4 and T5) and the Bromage score to the T4 sensory plane were recorded. The time from the start of anesthesia to the start of surgery was recorded, and patients were instructed to describe any pain using a visual analog scale (VAS), with 0 denoting no pain and 10 denoting the most severe conceivable pain.
An additional 5 mL of study solution was administered if bilateral sensory block was not achieved within 15 min of the epidural extension’s start. If these measures were unsuccessful in providing adequate analgesia, general anesthesia was considered.
Phenylephrine was administered to treat any intraoperative hypotension, defined as systolic blood pressure less than 100 mmHg or greater than a 30% drop from baseline. Toltesetron 5 mg was given intravenously to treat intraoperative vomiting, defined as more than two episodes without hypotension. Intraoperative pain, defined as a VAS score of 3 or higher, was managed with an epidural injection of 5 ml of the study solution (maximum total volume of 25 ml per patient) followed by intravenous esketamine at a dose of 0.25 mg/kg.
Primary outcome
The primary outcome was the time to onset of T4 block, defined as the time from the start of epidural extension to the loss of cold sensation at the T4 level. If the block did not reach T4 levels within 35 min after the epidural extension began, the onset time was reported as 35 min [6].
Secondary outcomes included the time to onset of T5 block, the modified Bromage score and sensory block at entry into the operating room and at the T4 level, time from induction to the start of surgery (defined as the time from the beginning of anaesthesia to the beginning of surgery), duration of surgery, volume of intraoperative intravenous fluids, vasoconstrictor medication requirements, and intraoperative pain management. Other secondary outcomes were Apgar scores at 1 and 5 min, VAS scores at the beginning of surgery, at delivery, and at the end of surgery, patient satisfaction scores (rated from 0 indicating extreme dissatisfaction to 10 indicating extreme satisfaction), incidence of nausea, vomiting, and shivering, and details of previous epidural analgesia.
Sample size
There are no existing data in the literature that clearly define a clinically significant reduction in onset time of anesthesia, a difference between the groups to be considered of interest was varied from 5–30% [6, 12, 21]. Based on the study, it takes 12.4 ± 1.1 min for 3% cloprocaine to provide a satisfactory level of anesthesia. A two-sided t-test was conducted with a test power of 95% and α=0.05. Assuming that the time difference between achieving satisfactory anesthesia level with 0.75% ropivacaine and 3% cloprocaine is within 10%, a total of 50 cases or 25 cases per group are required, taking into account a 10% loss to follow-up. G-Power software (version 3.1; Informer Technologies, Inc.) was used for the analysis.
Statistical analysis
The data were analyzed using SPSS 20.0 (SPSS, Chicago, Illinois, USA) and expressed as mean ± standard deviation and 95% confidence intervals (95% CI). For the primary outcomes, the differences between groups were expressed as median differences (95% CI). Differences between groups were compared using the unpaired t-test, and count data were compared using the X2 test or the Fisher exact probability method. Continuous variables with non-normal distribution were analyzed using nonparametric tests (Mann-Whitney U test). VAS scores were analyzed using generalized estimation equations. A two-sided p-value of < 0.05 indicates statistical significance.

留言 (0)