Study design and ethics statements
This single-centre clinical RCT was conducted at the Peking University Shenzhen Hospital, an affiliated hospital of Peking University located in Shenzhen, Guangdong Province, from June 2021 to December 2022. This study was approved by Professor Tao Wang, the chairman of the Clinical Research Ethics Committee of Peking University Shenzhen Hospital (IRB 2021[036]), and written informed consent was obtained from all participants. Before patient enrolment, this trial was registered with the Chinese Clinical Trial Registry (ChiCTR-TRC- 2,100,046,534, registration date: 21 May 2021).
Inclusion criteria
Potential participants were screened the day before surgery (or on the preceding Friday for those who underwent surgery on a Monday). Patients with obesity aged 18–65 years who underwent elective LSG were eligible for the study.
Exclusion criteria
Patients were excluded if they met any of the following criteria: (1) history of severe arrhythmia, myocardial infarction, or cardiac insufficiency (NYHA III/IV); (2) respiratory diseases; (3) hepatic/renal insufficiency; or (4) preoperative use of antiemetics.
Data collection
Detailed patient information was obtained after recruitment, including baseline demographic data, preoperative medical history, diagnosis at the time of admission, illness severity, and perioperative variables. After obtaining written informed consent, baseline data (demographic data, surgical type, and comorbidities) were collected.
Randomisation and blinding
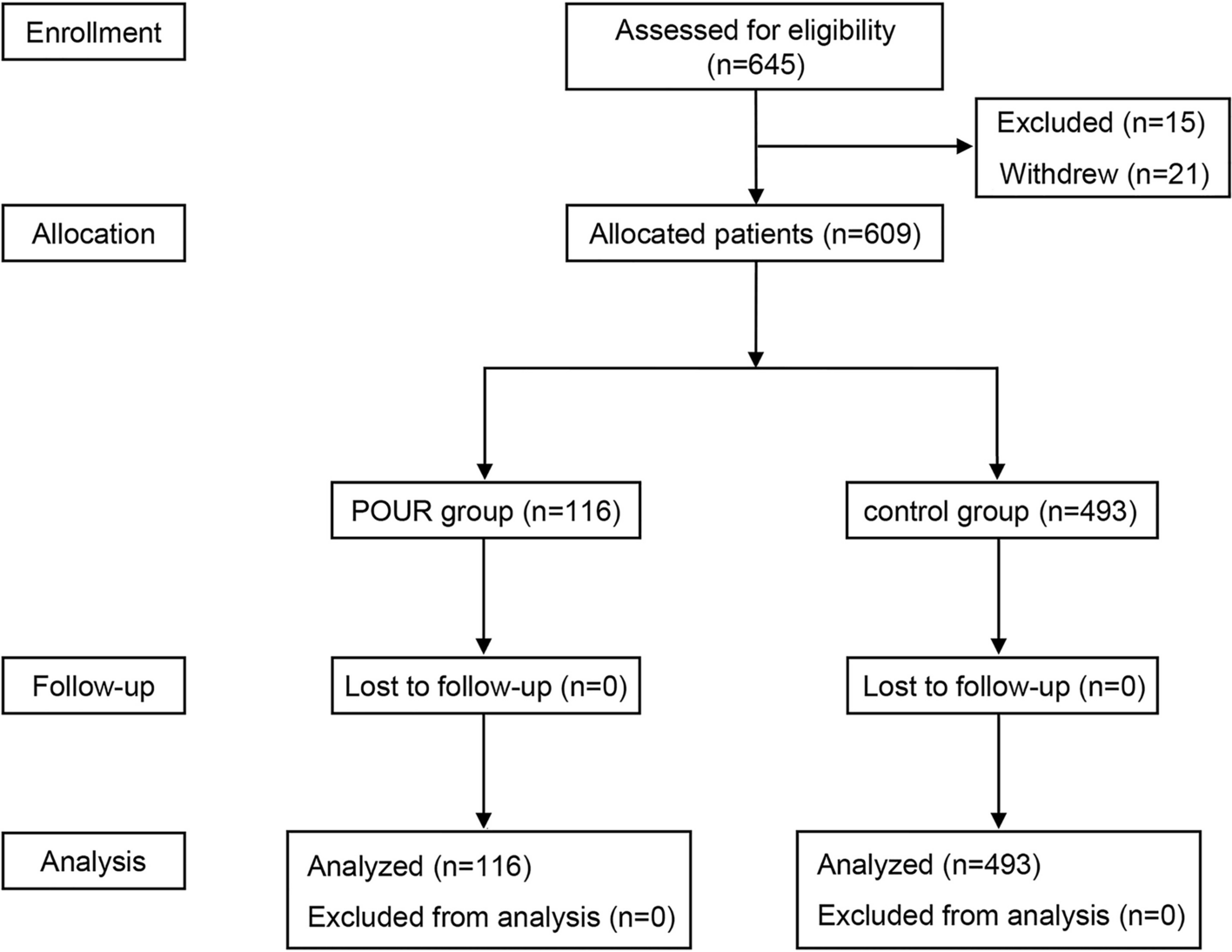
A biostatistician not involved in the data management and statistical analyses generated random numbers (at a 1:1 ratio) using SAS software version 9.2 (SAS Institute, Cary, NC, USA) with a block size of 4. The results of this randomisation were sealed in sequentially numbered envelopes and maintained until the end of the study by a study coordinator (Y.Y.) who was not involved in the data collection, perioperative care, or postoperative follow-up. During the study period, consecutively recruited patients received intra-operative OAP or CAP according to random number allocation by the study coordinator (Y.Y.). The investigators (B.L. and R.D.) collected intra-operative data for each recruited patient. The anaesthesiologists and investigators did not communicate with each other regarding the collected patient data. The patients and postoperative investigators were blinded to the group assignment.
Anaesthetic management
No premedication was administered; solid food and clear fluid intake were allowed until 8 h and 2 h preoperatively, respectively. Non-invasive blood pressure, peripheral oxygen saturation, electrocardiogram, bispectral index (BIS), and body temperature were continuously monitored. After preoxygenation for denitrogenation using the mask, propofol (1–2 mg∙kg− 1 total body weight), sufentanil (0.5 µg∙kg− 1 lean body weight [LBW]), and rocuronium (0.9 mg∙kg− 1 LBW) were administered for anaesthesia induction. Dexamethasone (10 mg i.v.) was administered as a prophylactic antiemetic after endotracheal intubation. The respiratory parameters were set as follows: tidal volume of 8 mL∙kg− 1 according to ideal body weight, respiratory rate of 10–12 times∙min− 1, and inspiratory-to-expiratory time ratio of 1:2. The respiratory parameters were adjusted to ensure a PETCO2 between 35 and 45 mmHg. Anaesthesia was maintained with sevoflurane (1.5–2.5%) and remifentanil (0.08–0.15 µg∙kg− 1∙min− 1) in the CAP group and propofol (6–8 mg∙kg− 1∙h− 1 LBW) and remifentanil (0.08–0.15 µg∙kg− 1∙min− 1) in the OAP group, keeping the BIS between 40 and 60. Sufentanil and rocuronium were administered to maintain adequate analgesia and muscle relaxation levels. Subsequently, 10 mg of azasetron was administered intravenously 30 min before the end of the procedure. For intra-operative fluid management in the CAP group, preoperative fluid deficit was estimated using the 4-2-1 rule based on the patients’ LBW and an 8-h fasting time. After the participants entered the operating room, half of the deficit was administered before induction using lactated Ringer’s solution. The other half was supplemented at the discretion of the attending anaesthesiologist to maintain a mean arterial blood pressure (MAP) > 65 mmHg and a urine volume > 0.5 mL kg− 1 h− 1. Whenever the MAP decreased to < 65 mmHg, rapid fluid infusion and vasoactive drugs (phenylephrine, ephedrine, or norepinephrine) were administered to maintain MAP at > 65 mmHg. In the OAP group, a pleth variability index (PVI) sensor (RainbowR2-25 a, Masimo Corporation, Irvine, CA, USA) was placed on the patient’s index finger to monitor the PVI continuously. The preoperative fluid deficit was corrected using the same protocol used for the CAP group. Half of the deficit was administered before induction using lactated Ringer’s solution, followed by a continuous infusion of crystalloids (2 mL kg− 1 h− 1). When the MAP was < 65 mmHg, the vasoactive drugs were promptly administered to maintain a MAP of ≥ 65 mmHg regardless of PVI. When the MAP was ≥ 65 mmHg, fluid responsiveness was considered with a PVI > 13%. Whenever the PVI was > 13% for 5 min, we administered a 250 mL bolus of colloid (hydroxyethyl starch 6%, Voluven®, Fresenius Kabi, Beijing, China). The dose was repeated every 5 min whenever the PVI remained higher than 13%. Subsequently, vasoactive drugs (phenylephrine, ephedrine, or norepinephrine) were administered to maintain MAP > 65 mmHg [11].
Postoperative prevention of PONV and pain management
When the patient returned to the ward, 10 mg of metoclopramide was administered routinely to prevent PONV. This was not considered an antiemetic treatment. If obvious PONV occurred in the ward, additional 10 mg of metoclopramide was administered as antiemetic remedy treatment. Postoperative pain was treated with intravenous flurbiprofen axetil (50 mg) or parecoxib sodium (40 mg) every 12 h for the first 24 h. Postoperative pain was measured using an 11-point numerical rating scale (NRS). Patients who experienced postoperative breakthrough pain received intravenous tramadol 100 mg.
Outcome assessments
The primary endpoints were the incidence and severity of PONV within 24 h postoperatively. The secondary endpoints included antiemetic treatment, time-to-first-remedy, incidence of moderate-to-severe pain, and postoperative length of stay (PLOS).
The severity of PONV was evaluated using a 4-point NRS, where a score of 0 indicated no PONV, 1 indicated mild PONV (nausea), 2 indicated moderate PONV (retching), and 3 indicated severe PONV (vomiting) [12].
Sample size
According to a retrospective analysis, the incidence of PONV in patients in the Peking University Shenzhen Hospital was 75% 24 h after LSG. The multimode intervention was hypothesised to reduce the absolute risk by 50%. With a test level of α = 0.05 and a test efficacy of 1-β = 0.80, each group required 55 patients. Consequently, 5% of the samples were lost, and 58 patients were expected in each group.
Statistical analysis
Initial data were collected using an Excel spreadsheet and transferred to an SPSS dataset for analysis. The Shapiro–Wilk test was used to analyse the Gaussian distribution of the quantitative data; P values < 0.05 were considered non-Gaussian distributions. Gaussian data were defined as mean and standard deviation (SD); non-Gaussian data were presented as median and interquartile range (IQR). The Gaussian data were analysed using the Student’s t-test, and the non-Gaussian data were analysed using the Mann–Whitney U test for significance. Categorical data were analysed using Pearson’s chi-square or Fisher’s exact test. P values < 0.05 represented statistical significance.







留言 (0)