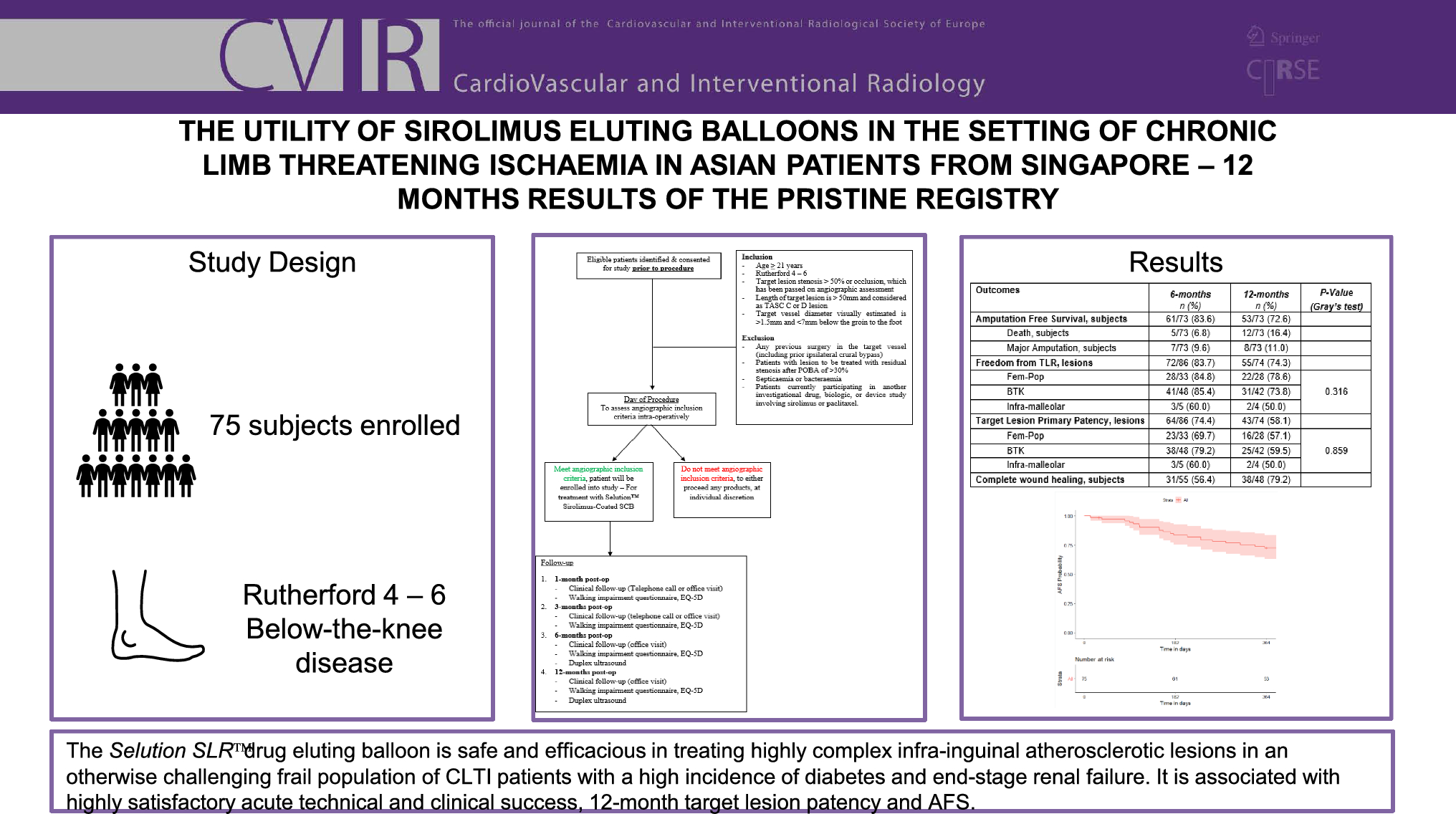
The PRISTINE registry is representative of everyday lower limb intervention practice for CLTI Asian patients in Singapore, who have long complex occlusive atherosclerotic lesions (mean of > 20 cm length) and heavy wall calcification. The data are relatively non-sanitized compared to RCTs, with liberal inclusion and few exclusion criteria. The strengths of the registry are that the follow-up of patients has been tight and prospective in nature with only few dropouts. The results demonstrated no peri-procedural early safety concerns, with no device complications or serious adverse events attributable to the device through to one year. It showed promising efficacy and clinical outcomes at 6 and 12 months, similar to other recent publications evaluating the performance of current SEBs on the market.[9, 11, 12] Despite high rates of diabetes mellitus, ESRF and moderate/severe vessel wall calcification, we have shown a 100% technical success rate (100%) and satisfactory 6- and 12- month primary vessel patencies of 74% and 58% respectively and freedom from clinically driven TLR of 84% (6 months) and 74% (1 year). An AFS of 84% and mortality rate of 7% at 6 months and 16% at 1 year are in keeping with what is expected from a challenging, frail population of patients with multiple co-morbidities.12-month primary patency rates for below-the-knee lesions and all-cause mortality rates were comparable to those reported in Stefanos et al.’s meta-analysis (59% vs 64% and 16% vs 9.0%, respectively). However, 12-month primary patency rates for above-the-knee lesions were lower in our cohort (57% vs 82.0%).[18] The SFA/pop subgroup is interesting in that the target lesion primary patency is lower than expected but fTLR is much higher. This may reflect SGH’s high threshold appetite for stenting an otherwise small Asian SFA/popliteal diseased artery because of concerns of stent complications.[19] The primary patency for these lesions were also lower compared to the XTOSI cohort of patients at both at 6 months (74% vs 88%) and 12 months (58% vs 79%).[12] XTOSI enrolled Asian CLTI patients with both fem-pop and BTK arterial lesions and used the MagicTouch PTA SEB (Concept Medical Inc., Florida, US), although their reporting definition was per patient rather than per lesion and the study included patients with intermittent claudication with less severe disease and co-morbidities on presentation. For BTK disease, the 6-month primary patency of 74% was comparable to MagicTouch.
A meta-analysis by Katsanos et al. reported significantly lower AFS in the paclitaxel-coated balloon arm as compared to plain balloon angioplasty, especially when high dose DCBs (3.0–3.5 μg/mm2) were used.[20] This was postulated to be due to distal non-target paclitaxel embolization resulting in micro-vessel occlusion, critical especially in the CLTI setting with minimal arterial reserve in the foot. One issue pertaining to the use of paclitaxel-based DCBs is the potential for the slow-flow phenomenon.[21] This was thought to be due to particulate embolization with the application of DCB with over 50% of drug lost down-stream reported.[22] This was thought to be a possible cause for the poorer outcomes with paclitaxel devices use reported in the meta-analyses by Katsanos et al.[23, 24] Early studies suggest no evidence of slow-flow phenomenon with the use of SEBs in the treatment of PAD, even for treatment of below ankle disease.[11] This was attributable to the micro-reservoirs of phospholipid polymer complex with the cell adherent technology of the Selution SLR™ SEB, which minimizes distal embolization.[21] Significant wound healing progress and improvement in ambulatory symptoms occurred with the balloon through 12 months. A complete wound healing rate of 79% is comparable, if not superior, with an open bypass salvage strategy [25] and previously published data on the use of paclitaxel coated balloons rates in lower limb endovascular revascularization for tissue loss.[26]
The results of PRISTINE may not be as impressive as those from PRESTIGE at the same time points, but this may be explained by the fact that PRESTIGE only included Rutherford 5 wounds whereas in PRISTINE, 22% had Rutherford 6 type advanced wounds and more than 50% of target lesions were TASC II D in nature. Furthermore, PRESTIGE only included tibial arterial lesions, whereas both femoro-popliteal and below the knee disease were allowed for PRISTINE, making the likelihood of mutli-level disease more likely to be treated with its intendent risks of restenosis and reintervention. While the initial results are encouraging and long-term follow-up is ongoing, the PRESTIGE Trial did not have a full range of SEB balloon sizes available to treat the entire vascular bed. PRISTINE included at least twice the number of patients to PRESTIGE, had the variable of multiple operators with differing peripheral vascular intervention experience using the technology and one of the aims was to determine whether complete revascularization of the affected vessel beds with SEBs will improve clinical outcomes as compared to treatment of only the tibial arteries. The results are encouraging in that they can reproduce similar results to PRESTIGE albeit with a bigger sample cohort with multiple proceduralists involved.
Limitations
PRISTINE’s limitations were its single arm, single centre, non-randomized nature and relatively small sample size with a self-adjudicated design. There was no comparator arm to draw to. No quantitative angiographic analysis was performed to look at exact lesion lengths, reference vessel diameters and luminal gain post angioplasty for each target lesion. Furthermore, there was no core lab adjudication for artery patency at follow-up and Duplex ultrasound was the modality of choice to assess TLPP, with its inherent limitation of operator bias. Furthermore, Duplex follow up was not core lab adjudicated. Whilst convenient, there is also no consensus to accurately determine vessel patency using Duplex ultrasound for BTK lesions.
Although this registry did not raise any early safety concerns, the data presented is through to one year only. Together with the small number of patients included, no conclusions can yet be made regarding the long term safety of SEBs. Another limitation was the attrition rate for primary patency assessments at 6 and 12 months; although mortality and major lower limb amputations were the main reasons for the drop out, which are expected for this type of frail cohort with multiple co-morbidities.
Furthermore, the wound care practiced at SGH for CLTI diabetic foot is relatively unique whereby the wound debridement and post-operative care are performed by the vascular specialist themselves in a timely manner with all the latest wound products and technology available to promote tissue granulation, which may limit the generalizability of our results.



留言 (0)