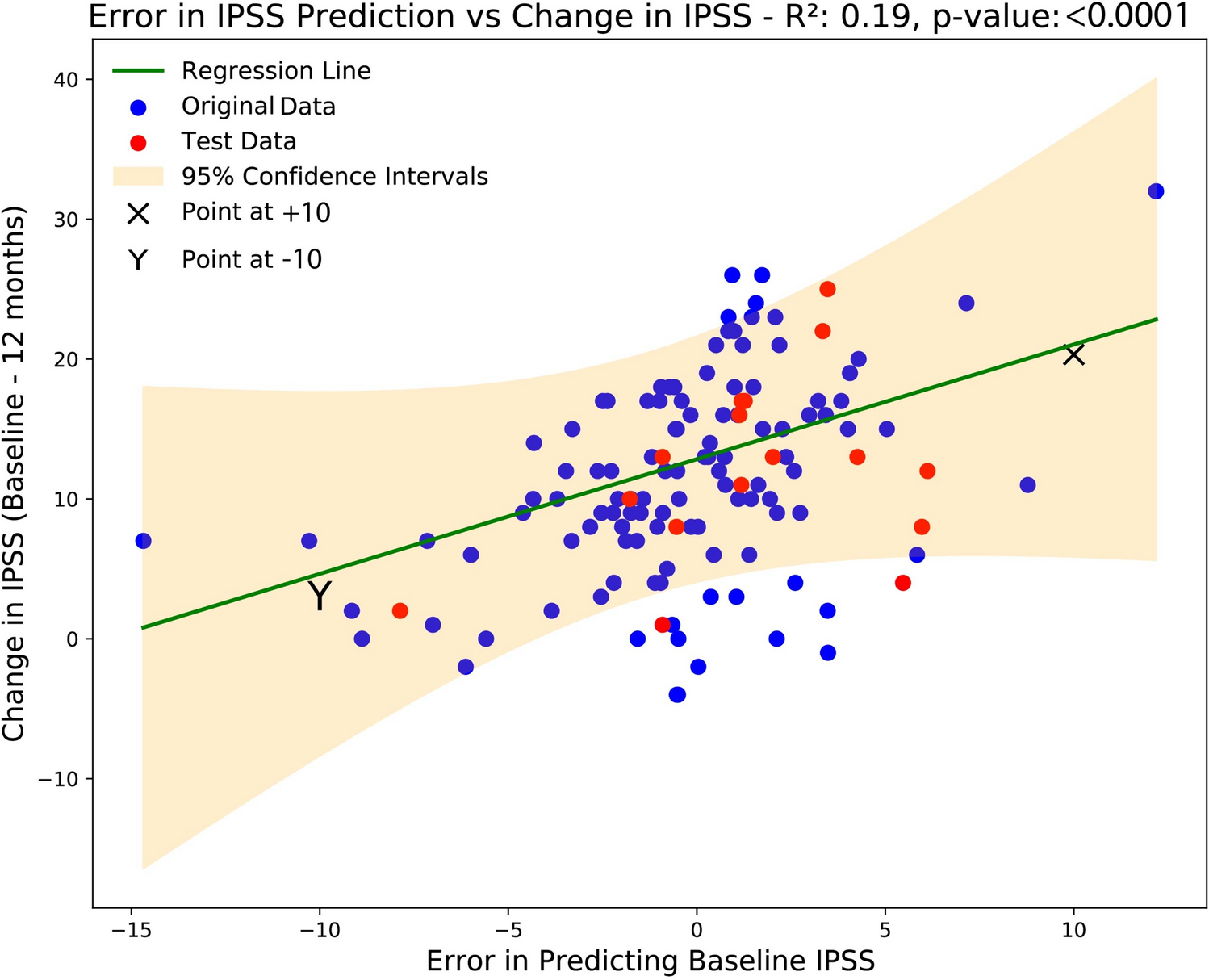
Our findings suggest that despite using a limited dataset, ML models can be used with routinely collected pre-procedure data to predict the change in IPSS at 1 year following PAE. Interestingly, the most effective way to predict patient outcome was by using purely objective clinical measures to create a ‘model-generated baseline IPSS’. The degree of error between this and the patients’ actual observed IPSS (termed the ‘model-generated baseline IPSS error’) significantly correlated with the ‘change in IPSS’ at 1-year post-procedure and can be used to predict individual patient outcomes with reasonable accuracy.
This finding might reflect a difference between objective and subjective measures of symptoms and points towards a potential psychological element of symptom evaluation through IPSS scoring. Certainly, patient expectations prior to procedures have been shown to significantly influence outcomes. Patients’ beliefs and perceptions about the forthcoming procedure can shape their psychological response, which in turn can influence physiological outcomes, and overall satisfaction with the procedure. For instance, a study by Ellingsen et al. [14] demonstrated that negative expectations could intensify the experience of pain and discomfort. Moreover, when patients hold positive expectations, they are often more compliant with pre- and post-procedure instructions, leading to improved outcomes and decreased complication rates. Indeed, the opposite also applies, in that patients who were adequately informed and thus had clear expectations had shorter recovery times report higher satisfaction rates [15]. This emphasises the importance of effective patient education and setting appropriate expectations to optimise both subjective and objective outcomes in interventional radiology. However, the objective nature of urodynamics is also controversial, e.g. there is some evidence that Qmax is effort dependent and influenced by intervention [16, 17]. Therefore, this is a complex area and needs to be interpreted carefully within this context.
Given the therapeutic intent of PAE is to provide symptomatic relief, it is likely that a combination of psychological and biological factors would lead to symptom improvement. Thus, it remains of pertinent clinical utility to continue using both objective and subjective variables as inputs for any future developed model.
We also found that including a combination of routinely collected variables, notably, prostate volume and urodynamic variables can be used for prediction and is in line with previous studies that have identified prostate volume as a significant predictor of clinical success. Patients with larger prostatic volumes, often above 80 cc, have shown better symptomatic relief post-PAE as compared to those with smaller prostates [18]. This also applied to our model, in which, increasing prostate volume predicts greater IPSS improvement. (We explored this by increasing prostate volume with our tool and observing the predicted change in IPSS rising.) However, critically, it was not this single variable alone that contributed to model performance. Instead our study utilised a combination of factors to predict IPSS outcomes, thereby benefiting from potential performance gains from variable combinations [19]. Machine learning also provides a way in which clinical decision support tools can be improved on subsequent iterations, once additional data are trained, as well as being able to be deployed through interfaces such as ‘Rshiny’ [12].
Notably, our model demonstrated applicability to a separate, blinded dataset (Dataset 2), enhancing the generalisability of our findings. This underscores the potential benefits of establishing a more comprehensive registry of PAE patients. Such an expanded registry could significantly improve model performance, offering deeper insights into patient outcomes and optimising treatment strategies.
Whilst these initial results are promising, it is important to acknowledge the limitations of our study. Firstly, the sample size might mean our models are not representative of the general populations. However, some generalisability was assessed by testing our models on a blinded independent dataset and in part by being trained on multicentre level data. We were also restricted in selecting variables that had full data, as most ML algorithms require complete data. Whilst a single radiological parameter (namely prostate volume) has been used in our models, other radiomic markers might be relevant and imaging data has not been fully utilised. Any future work would also include this readily available and now routinely collected data type, especially given the advantages of performing pre-procedure CT for planning [20]. In addition, clinical measures from formal urodynamic studies were an important component to the ML model. As many centres do not routinely perform urodynamics prior to PAE, this reduces the wider utility of the model and findings.
Furthermore, we emphasise the use of these models as a tool to support clinicians in their decision-making and not to be used as a triaging software independent of clinical oversight.



留言 (0)