In the sections that follow we discuss the properties of the physical and virtual control rooms according to the dimensions introduced above, and we consider the theoretical approaches taken to establish and operate such centres. Given that human factors issues are only just starting to be systematically addressed in the establishment and operation of HCCCs, we cover a broad range of issues relating to the human role in HCCCs that contribute to their success or otherwise.
Physical Control Centres
The decision to co-locate patient management functions is often motivated by the perception of system-wide inefficiencies, reflected in increased times for patient admission, transfer and discharge, ED overcrowding and increased delays, increased ambulance diversions, delayed bed assignment, delays in operating room discharges, and decreased patient satisfaction [40,41,42].
Eight papers discuss the benefits of physically co-locating staff with respect to patient management parameters [16, 23, 41, 43,44,45,46,47]. For example, Kane et al. analysed the existing patient capacity in a health care system and set out to enhance patient flow by reducing patient boarding in the ED, and improving critical transfer care processes from outside facilities [41]. They created a centralised, physical command centre that helped staff streamline work, share best practices, and prioritise projects. Hospital occupancy increased from 85 to 92% and ED delays decreased from 9.7 h to 6.3 h. Further, Davenport et al. showed that the centralisation of patient transfer and flow processes across two hospitals led to a 19% increase in transfer volume, improved ICU bed availability and an annual cost saving of US$1.5M [43]. Finally, Lovett et al. showed that implementing a patient flow management centre in a multicampus academic health system improved ED metrics such as a reduced number of ambulance diversions time from ED entry to seeing a provider, environmental services turn around time (and bed assignment time) and the number of patients who departed without being seen. These improvements occurred despite increased admissions, transfers and emergency department visits, and resulted in substantial cost savings. Reduction in leaving without being seen rates was estimated to save $2.1 million per annum [40].
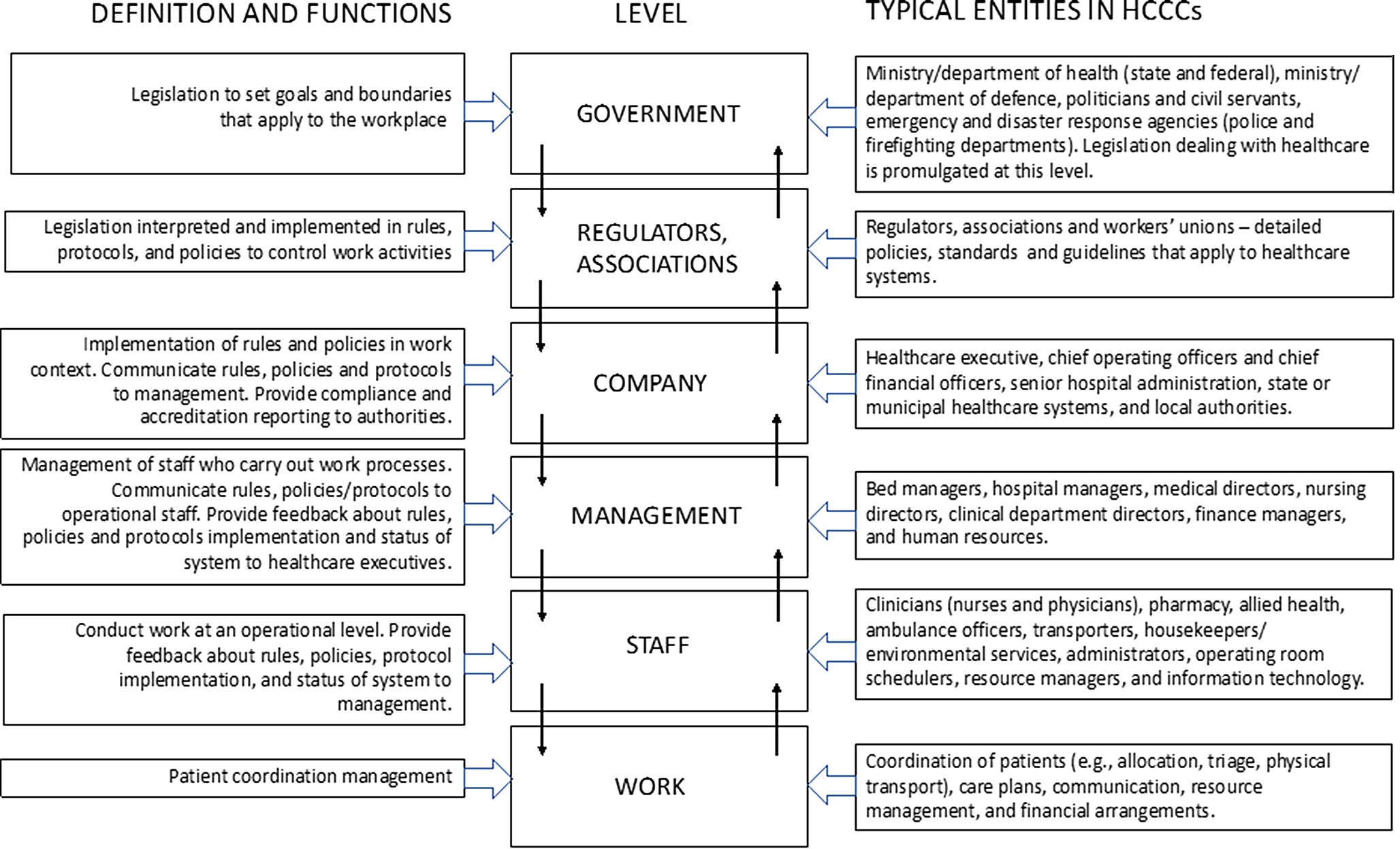
As Table 2 shows, the HoCCs included in the review deal principally with BAU, where the most commonly-involved organisational levels are staff/units and hospital management. Rules and routines for handling BAU naturally devolve to lower levels of the RMF. However, control rooms need to be agile to deal with a surge in patient presentation, which varies depending on circumstances such as time of day, day of the week, seasonality or surge events [48,49,50,51,52,53,54,55]. If an abnormal event leads to increased patient presentations, a HoCC can be transitioned to a surge management model. For example, one paper describes how a HoCC transitoned to handle surges in a paediatric hospital [55]. Other papers describe specific incidents, including the management of patients with infectious diseases such as COVID-19 [49, 50, 52, 54, 56,57,58] and Ebola [59], natural disasters such as hurricanes or tsunamis [60,61,62,63,64,65,66,67], manmade disasters such as radiation incidents [68], food borne disease outbreaks [69], mass casualty events such as terror-related events [70, 71], bomb threats and transport accidents [72]. As situations move beyond BAU to MCM, ER and SM, the involvement of higher levels of the RMF up to government itself is more firmly represented. This is to be expected when a HoCC extends its focus to more widespread or critical incidents and more agencies become involved.
At the most extreme levels, ICCs are established to deal exclusively with situations beyond BAU—mostly MCM, although we found two papers covering ER [73, 74] and three covering SM [56, 57, 75]. ICCs are usually closely coupled with outside stakeholders and agencies who manage other aspects of incident response. Key staff need to be co-located to receive timely and relevant information, communicate quickly and maintain situation awareness to enhance decision-making. Formal communication pathways and protocols across organisational levels are necessary for coordinated and efficient incident response. We found a balanced representation of organisational levels in the RMF for ICCs, as would be expected given the multi-agency coordination required for incident response.
Virtual Control Centres
When managing patients on a BAU basis, not all hospital systems create a full-scale physical control room. This may be due to cost and resource constraints, or satisfaction with how patient flow functions are being managed virtually [23, 76]. In virtual control rooms, staff tend to be dispersed across the system and they communicate electronically, yet they have similar staff complements, goals, and tasks to physical control rooms.
As Table 2 shows, most of the virtual HCCCs included in the review deal with BAU, with a few dealing with ER [77,78,79,80] and one with SM [51]. Again, the levels of the RMF most involved in BAU are staff/units and management. Existing hospital resources can be used to improve patient flow management by improving communication about patients’ care plans and discharge needs [81]. Other initiatives include the introduction of software products such as bed management systems and electronic dashboards [81,82,83,84,85,86,87]; the establishment of a bed management team [86]; regular bed management/safety huddle meetings [81,82,83,84,85, 87, 88]; the appointment of a transfer coordinator/team [48, 82, 89]; and expedited discharge times [82]. Moreover, introducing a logistic management program with a dedicated logistics manager to coordinate patients improved patient assessment time and length of stay metrics in an ED [82].
Four papers addressed the use of a virtual control structure to manage emergency response activities relating to burn casualties [77, 80] and military patients [78, 79]. Only one paper described a virtual control structure for surge management of adult and paediatric patients with COVID-19 and the challenges of stepping up to a higher tempo of work [51]. No paper described the application of a virtual control structure for the management of mass casualty events.
Systems-Wide and Human Factors Approaches
Several studies noted that a system-wide approach is needed to improve patient management, while taking into account competing hospital priorities [11, 41, 44, 45, 49, 55, 82, 84, 90, 91]. The articles relied on various systems-based frameworks for investigating patient management, including the concept of High Reliability Organisations (HRO) [16, 43]; lean management models [23, 83, 86, 90]; Plan-Do-Study-Act [49, 75, 85, 90]; quality improvement (QI) [83, 85, 92, 93]; process mapping/tracking [78, 81, 83, 85]; Ishikawa Diagrams [78, 83]; and Design-Measure-Analyse-Improve-Control (DMAIC) [83]. One paper described a systems engineering approach to analyse and maximise capacity in one health system for BAU, which resulted in the establishment of a centralised capacity command center [41]. Two studies detailed a systems thinking approach to optimise the response and preparedness plan for pandemics [49,




留言 (0)