In a large retrospective sample of patients admitted to the PACU at a single academic medical center, we demonstrated an association between a mobile electronic PACU order reminder system and more timely order entry. Use of the system was associated with a greater percentage of patients arriving to the PACU with orders entered and, in those without preexisting orders, was associated with more rapid order entry during the PACU stay. In a post-hoc sensitivity analysis, order placement prior to PACU admission was associated with shorter PACU duration and decreased odds of both higher PACU pain scores and the incidence of multiple administrations of antiemetics.
Interestingly, while the reminder system was associated with increased odds of timely order placement, and on-time order placement was associated with shorter PACU durations, we found that patients whose attending utilized the system had longer median PACU durations than those who didn’t. However, this discrepancy is likely related to an interaction with one or more confounding variables. For example, we found that, other than on-time order placement, PACU length of stay was also associated with sex, race, height, weight, ASA class, case level, anesthesia duration, and provider-specific variables.
In the logistic regression analysis, the following provider-level factors were additionally associated with the placement of PACU orders prior to PACU admission: attending change during the case, in-room provider change during the case, and in-room provider with ordering privileges present during the case. Interestingly, these factors had variable effects on the outcome. A change of attending or the presence of an in-room ordering provider were both associated with greater odds of order placement, possibly because the oncoming ordering provider used the handoff as a cue to place the orders at that time. Conversely, a change in the in-room provider was associated with decreased odds of order placement. Each of these findings may be due to the distribution of responsibility for order placement amongst a group of providers, each of whom may have assumed orders were placed by another team member.
To account for other factors which may have affected the likelihood of timely PACU order placement, we additionally adjusted for anesthesia duration, case urgency, and patient ASA physical status. As expected, sicker patients and higher case urgency were associated with a decreased odds of order placement prior to PACU admission, while longer anesthesia time was associated with increased odds.
Over recent decades, the evidence supporting CPOE and electronic alerts and reminders in varying healthcare environments has grown [5, 6]. In the operating rooms, alerts embedded in anesthesia information management systems (AIMS) have been shown to improve compliance with antibiotic administration, treatment of hyperglycemia [5], and more. The transition to PACU, however, offers an additional opportunity where electronic alerts may provide operational or patient benefit. The added challenge of alerting a provider who is not actively working within the AIMS was overcome, in this case, via mobile device push notifications. Our study demonstrates a proof-of-concept that such technology can successfully reach clinicians and impact their behavior, with the potential to translate this method to other areas of healthcare.
It is also important to note that frequent push notifications can contribute to provider fatigue, leading to increased likelihood of being ignored. We attempted to mitigate these issues by allowing clinicians to add personalized user preferences and opt out of specific types of reminders. While data on changes to user preferences over time are not available, anecdotally our attending anesthesiologists have found this functionality useful.
This study has significant strengths including the inclusion of a large, diverse surgical population at a tertiary medical center operating room. The large sample size allowed increased power to detect significant differences between cases in which an order reminder system was or was not used for PACU order placement. Furthermore, the robust data collection procedures and analytic plan are easily replicated, leading to increased trustworthiness of results.
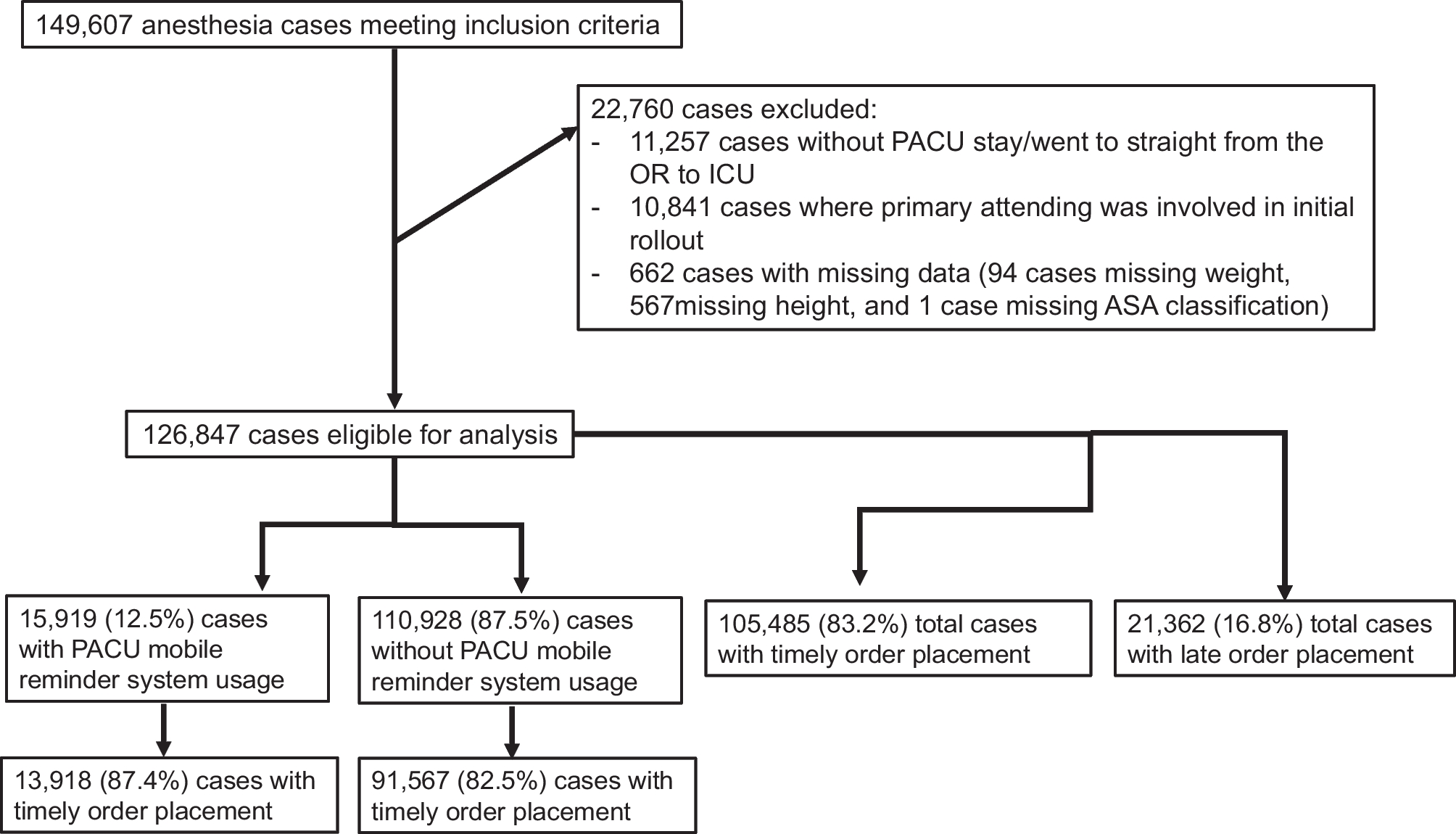
However, there were also several limitations. First, due to its single-center, retrospective design, the results of this study may not be generalizable to other patient populations. Also, we defined reminder system use as positive if the attending anesthesiologist received at least one push notification on the day of the surgery. We were unable to directly link reminders to individual surgical cases, and so our classification of cases likely included some false positives (cases in which the attending received an alert on the same day as, but not directly linked to, a specific case). Nor were we able to confirm acknowledgement of the reminder by the clinician. As a suggestion for future quality improvement initiatives, a more precise definition of system usage and reminder receipt could eliminate such bias. Similarly, the removal of cases with missing data is another potential source of bias. However, we feel that due to the relatively small number of cases with missing covariate data (< 1%), any bias that may be introduced is negligible.
In conclusion, in this single-center retrospective study, we found that an electronic reminder system was associated with timelier PACU order placement, which in turn may lead to improved patient outcomes.




留言 (0)