
記住我

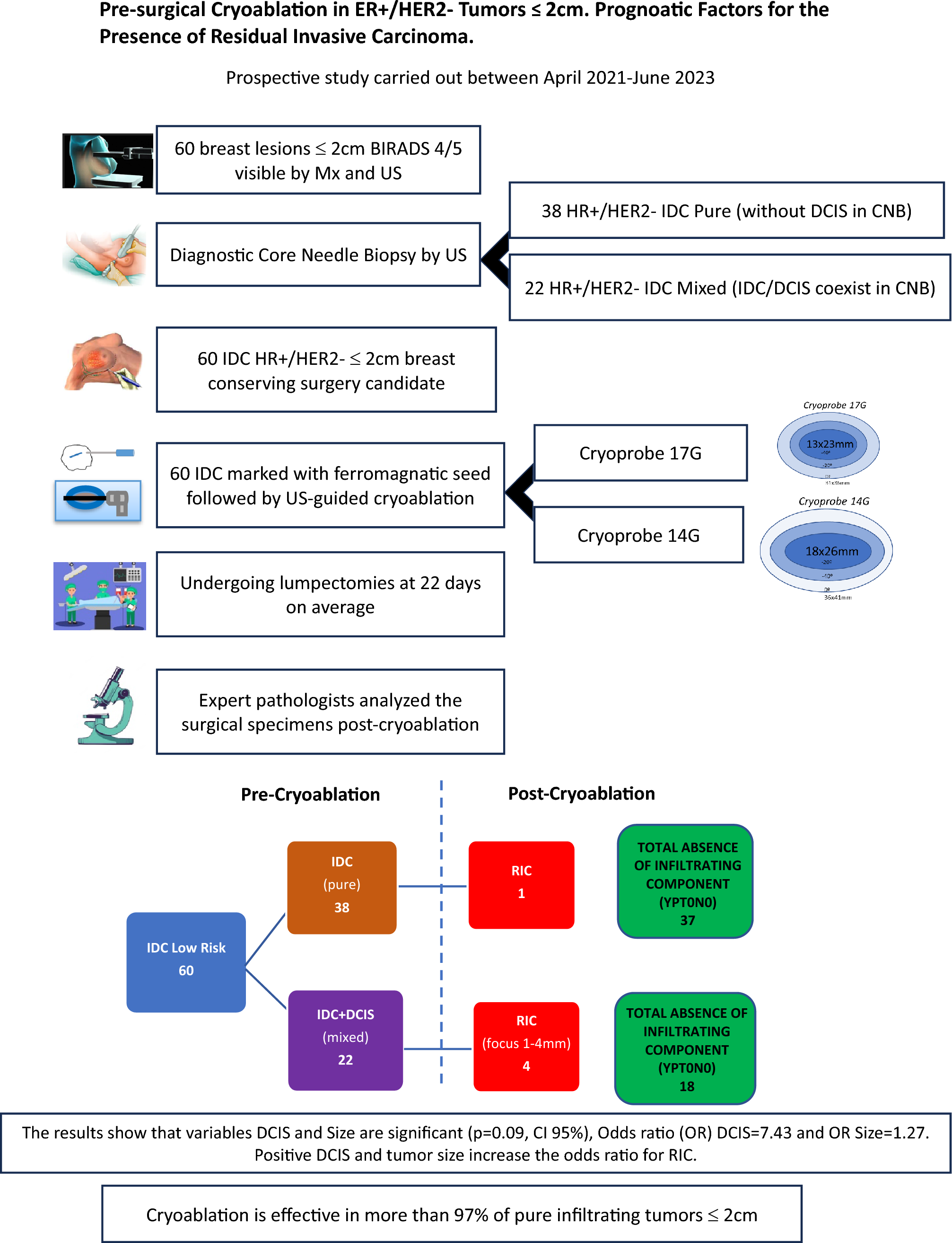

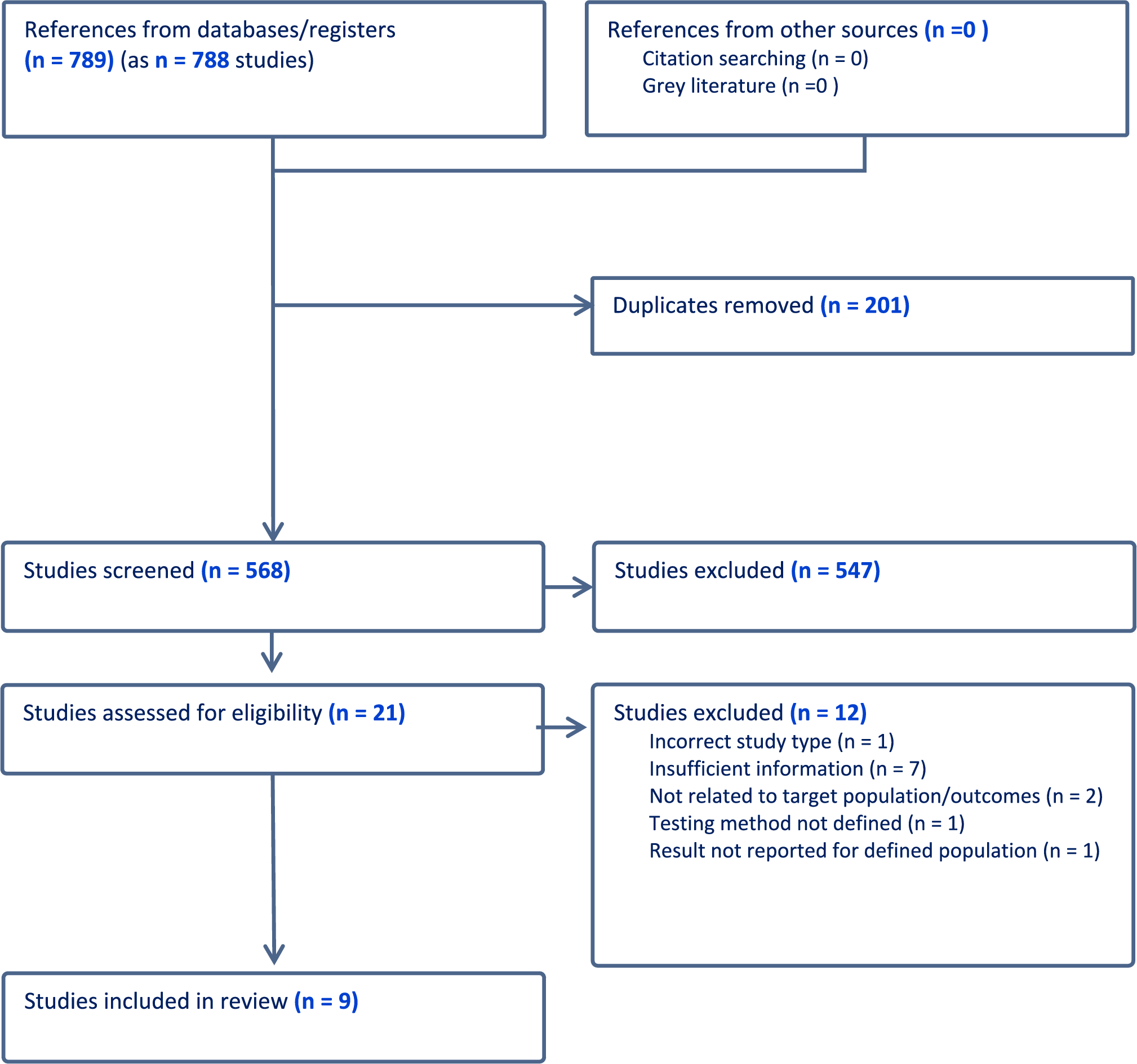

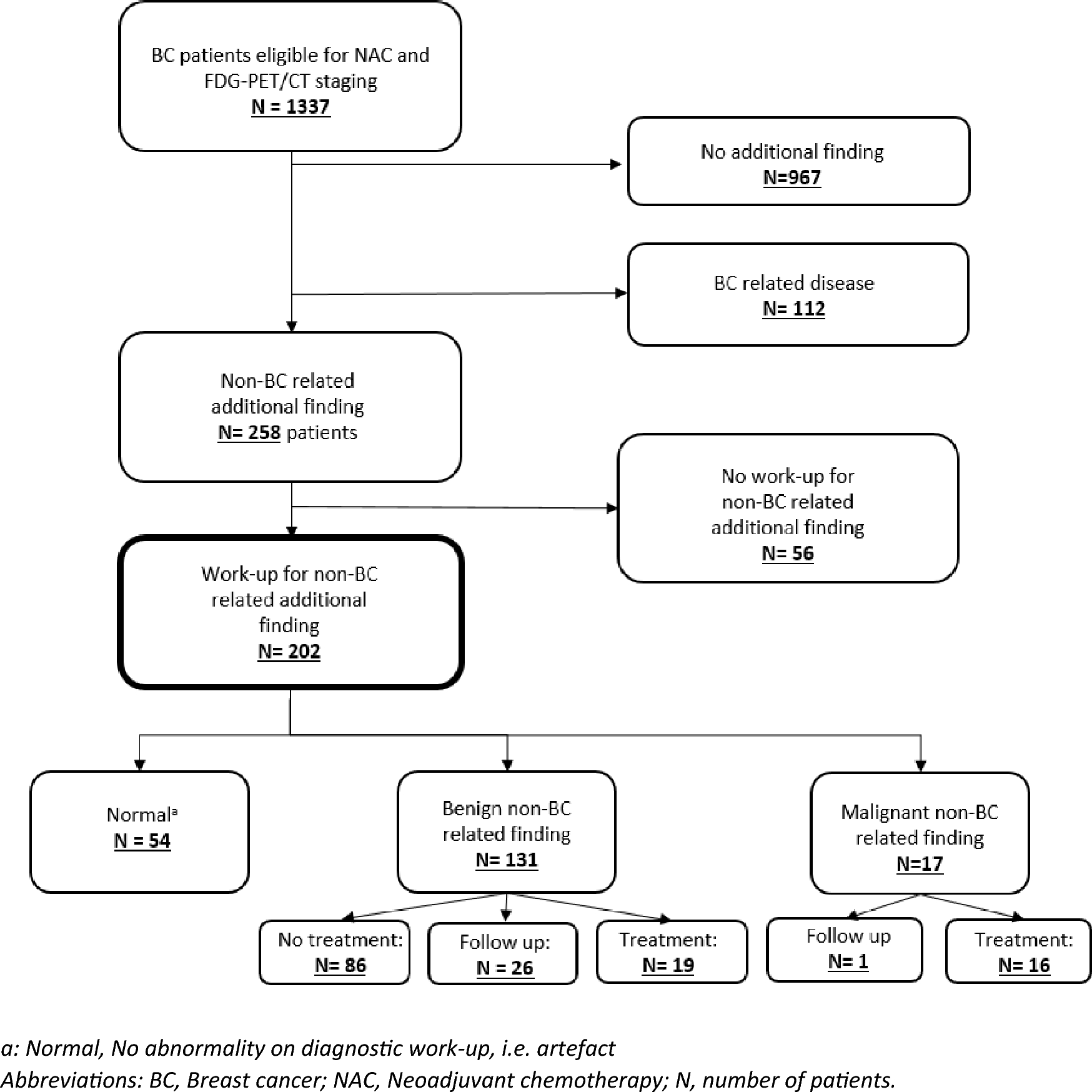
The PRISMA flow diagram (Fig. 1) depicts 789 citations identified, of which 201 were duplicates and 547 excluded on title and abstract screening. After full-text review, nine studies [22, 28,29,30,31,32,33,34,35,36] met the inclusion criteria (See Table 1). Of these, three were RCTs, two case–control studies, and four single-arm studies. Oestrogen testing methodology is outlined in Table 2.
Fig. 1 Table 1 Summary of study characteristicsTable 2 Summary of oestrogen testing methods
Table 1 Summary of study characteristicsTable 2 Summary of oestrogen testing methodsMethods used to measure oestradiol and oestriol in selected studies included mass spectrometry and immunoassays; several studies used more than one with variable concordance [22, 33]. Mass spectrometry detected oestradiol levels down to a lower limit between 1.0 pg/mL and 3.0 pg/mL [22, 29, 33,34,35,36]. Immunoassays such as ELISA (enzyme-linked immunosorbent assay), ECLIA (enhanced chemiluminiscence immunoassay) and RIA (radioimmunoassay) had lower detection limits ranging between 0.8 pg/mL and 10 pg/mL [22, 28, 30, 32,33,34, 36].
The highest quality and largest study was Sanchez-Rovira et al.’s trial of vaginal oestriol [35]. Sixty-one women with HR+ EBC taking an AI for > 6 months were randomised to a 0.005% oestriol gel (50mcg oestriol per application) or placebo moisturising gel daily for 3 weeks then twice weekly for 9 weeks. Serum oestrogen levels were measured at baseline, 3, 8, and 12 weeks via ultrasensitive LC-MS (detection limit of 3 pg/mL for oestradiol and 1 pg/mL for oestriol) [37]. There was no significant rise in E2 detected. A small rise in E3 was detected in the treatment group in the first 3 weeks returning to same level as the placebo group by 12 weeks (median, [interquartile range IQR], E3 = 0.5 pg/mL [0.5 to 7.3] in the treatment group and 0.5 pg/mL [0.5 to 0.5] placebo group, p = 0.140). Oestrone, follicle stimulating hormone (FSH) and luteinising hormone (LH) had no significant changes detected at any timepoint.
The REVIVE study [33], an ongoing open-label RCT, reported serum hormone levels for the first eight participants. This study compares a vaginal oestradiol ring (Estring®) which releases approximately 7.5mcg oestradiol daily for 90 days to a polycarbophil-based vaginal moisturiser (Replens ™) in women with HR+ EBC taking an AI. Two different ELISA kits were used to quantify oestradiol (E2) with a detection limit of 3 pg/mL. There was concordance between two ELISA kit measurements for 5/6 patients, but one had different results: E2 < 3 pg/mL versus E2 67 pg/mL. Samples from three patients were analysed using LC-MS/MS with a detection limit of 1 pg/mL. The values of E2 between different testing methods (ELISA and LC-MS/MS) varied markedly. One patient had higher readings of E2 on both ELISA kits compared to LC-MS/MS, and the degree of elevation varied between the two kits. Another patient had elevation in E2 at 2 weeks on LC-MS/MS, not detected on ELISA. The third patient was taking exemestane, an AI known to cause aberrant results via immunoassays due to cross-reactivity [20, 38]. Her results showed the anticipated rise in E2 on ELISA, but corresponding LC-MS/MS testing showed an elevated level of E2 at baseline but levels < 2 pg/mL at all other timepoints, attributed to a laboratory error. Although the RCT design is sound, this sub-study is fraught with issues: small sample size (N = 8), heterogeneity of testing methodologies, and discordant results.
Melisko et al. [22] conducted a randomised open-label phase 2 study comparing vaginal testosterone cream to a vaginal oestradiol ring (Estring®) in 76 women with HR + EBC on AI for > 30 days. The vaginal testosterone cream was used daily for 2 weeks then three times per week for 10 weeks for the first 24 participants then changed to three times per week for the 12-week study duration for the subsequent 12 participants. Both RIA and ultrasensitive LC-MS methods were used to measure oestradiol (E2) with a detection limit of 3 pmol/L (0.82 pg/mL) for RIA and no reported detection limit for LC-MS. The authors predefined < 10 pg/mL as the expected postmenopausal level of oestradiol, and the primary safety endpoint was defined as < 25% of participants having a persistent elevation of E2 (> 10 pg/mL and at least > 10 pg/mL above baseline on two consecutive blood tests more than two weeks apart) and was met for both arms in this study. 63 participants had E2 measured with both methods and surprisingly of these, 25 (40%) had baseline E2 above the 10 pg/mL threshold with LC-MS and 9 (14%) with RIA. In the oestradiol ring arm, 4/35 participants had a transient rise in E2 (range 11–29 pg/mL) but none had persistent elevation. No differences were detected in mean E2 levels between LC-MS and RIA at baseline (17.7 [SD 28.5] pg/mL and 17.9 [SD 44.1] pg/mL, respectively) or at week 4 (7.8 [SD 15.0] pg/mL and 2.9 [SD 13.4] pg/mL, respectively). There was some variability of reported E2 levels between RIA and LC-MS on review of matched samples, but discordant E2 elevation was rare (2/63 participants with matched samples). Similar to REVIVE [33], Melisko et al. found that LC-MS was more likely than RIA to detect an early rise in E2, 19% of participants had elevated E2 at 4 weeks with LC–MS vs. 1.5% with RIA. This study had a reasonable sample size, with most patients (63/76) having matched samples, allowing greater reliability of concordance assessment for testing methods. Although very discordant results were rare, there was still variability and RIA failed to detect early rises in E2 which were detected with LC-MS.
A prospective, open-label, single-arm study by Kendall et al. which showed a persistent rise in oestradiol (E2) levels, [32] is often used as a basis for concern regarding safety of vaginal oestrogens. In this study, six women with HR+ EBC on AI for > 6 months used a 25mcg vaginal oestradiol pessary (Vagifem®) daily for two weeks, then twice weekly for 10 weeks. Oestradiol (E2) was measured using RIA with a detection limit of 3 pmol/L (0.82 pg/mL). One participant on exemestane had high baseline levels of E2 attributed to cross-reactivity with immunoassays [38]. E2 levels increased at two weeks in 5/6 participants (from median 0.82 pg/mL at baseline to 19.61 pg/mL) and decreasing to median 4.36 pg/mL at 4 weeks and stayed at this level for most participants. However, two participants had persistently raised E2 when tested between 7 and 10 weeks (37.32 pg/mL and 59.65 pg/mL), one of whom was on exemestane. This study has several limitations including a very small sample size, no randomisation, heterogeneity in testing schedules, and variable reported oestrogen levels. The study also used a 25mcg oestradiol pessary, which has been subsequently replaced by a lower dose 10mcg preparation (Vagifem Low®).
Donders et al. [29] enrolled 16 women with HR+ EBC on AI for > 6 months to take a vaginal tablet containing 100 million acidophilus KS400 and 0.03 mg oestriol (Gynoflor®) daily for 4 weeks, then three times per week for 8 weeks. The authors used a highly sensitive GC-MS to quantify oestradiol (E2) and oestriol (E3) with a detection limit of 1 pg/mL and 10 pg/mL, respectively. As expected, there was no rise in E2 (as oestriol does not back convert to oestradiol [17, 18]), but there was a small transient rise in E3, most pronounced after the first dose. Oestrone, LH, FSH and sex hormone-binding globulin (SBHG) were tested, with no change detected except in FSH which had a small but significant decrease at 4 weeks. Again, this study is limited by a very small sample size and its single-arm design.
A short study by Pfeiler et al. [34] assessed use of oestriol 0.5 mg pessaries (Ovestin®) daily for two weeks in 10 women with HR + EBC on anastrozole. Oestradiol (E2) was quantified at baseline and 2 weeks using both ECLIA (detection limit of 10 pg/mL) and GC-MS (unreported detection limit). No significant change was reported for E2 or E3, but mean FSH and LH levels decreased significantly from baseline to 2 weeks (LH − 10.8%, p = 0.02; FSH − 12.8%, p = 0.01). This is a very small, single-arm study of two-week duration; thus, the duration of effect on FSH and LH remains unknown. Both ECLIA and GC-MS were performed, but detection limits were much higher for ECLIA than in other studies, so small rises in E2 could have been missed.
Biglia et al.’s [28] non-randomised three-arm study compared 0.25 mg oestriol cream, 12.5mcg oestradiol pessaries (Vagifem®), and a vaginal moisturiser (Replens™) in 26 women with HR + EBC on endocrine treatment. Unlike other studies reviewed, women on AI were not permitted in the vaginal oestrogen groups (but permitted in moisturiser group). RIA was used to quantify oestradiol (E2) with a detection limit of 5 pg/mL. No significant difference was found in E2 levels from baseline to week 12 or additionally, in E3, E1, LH, FSH, testosterone and SHBG. Although there were no reported issues with E2 RIA testing, the lower detection limit of 5 pg/mL is not as sensitive as methods used in other studies. Given most patients were not on an AI, the impact of small rises in oestradiol is less concerning.
Wills et al.’s prospective case–control study enrolled 48 women with HR+ EBC or an increased risk of developing BC (all on endocrine therapy) and compared cases of those on vaginal oestrogens for > 3 months (25mcg oestradiol pessary twice weekly or vaginal oestradiol ring inserted every 90 days), with a no vaginal oestrogen control group [30]. Oestradiol (E2) levels were measured using RIA with a detection limit of 3 pmol/L (0.82 pg/mL). For women using oestrogen pessaries for > 3 months, pre-insertion levels of E2 were not elevated compared to controls, although 12 h post-insertion E2 levels were raised. For those using the oestrogen ring for > 3 months, pre-insertion mean E2 levels were already elevated compared to controls suggesting a persistent elevation in E2 in this group. This study implemented a novel approach testing oestrogen levels pre- and post-insertion in women who had used vaginal oestrogens for > 3 months, with the intent of capturing whether persistent elevation in oestrogens occurred before insertion and after.
Streff et al. conducted a prospective study of vaginal oestradiol rings (Estring®) in women with HR+ EBC on AI [36]. This study included 8 prospective participants and 6 retrospective participants who had oestradiol (E2) quantification via tandem mass spectrometry or ECLIA with a variety of laboratories and reference ranges. Baseline E2 levels were in the expected range, but after commencing the oestradiol ring, 6/8 prospective participants had a transient rise in E2 (at week 4) which returned to baseline levels by week 16. The study quality was low due to small sample size, heterogeneous testing methods and no clear definition of the detection limits used.
Due to the heterogeneity of studies included in this systematic review, a formal bias assessment was not possible.
留言 (0)