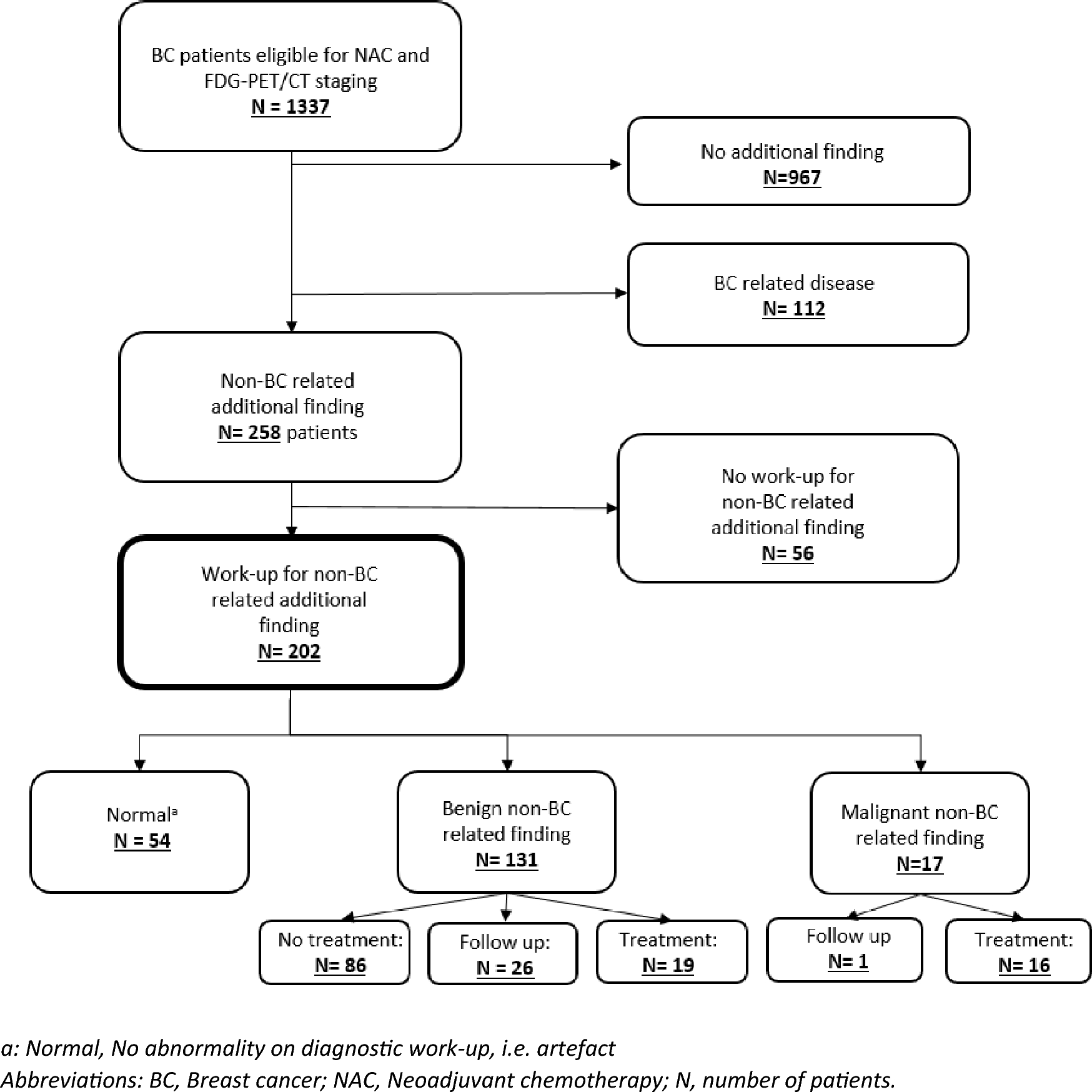
This study investigated the clinical implications of non-BC-related additional findings on FDG-PET/CT in patients eligible for NAC. We observed that 28% (370/1337) of the patients had additional findings, of which 202 patients (15%) had a non-BC-related finding resulting in a total of 318 extra diagnostic examinations. In over half of these 202 patients an invasive diagnostic procedure was performed during work-up; imaging plus biopsy (34%), endoscopy (15%), and endoscopy plus biopsy (14%). Ultimately, only a small number of 17 (8%) patients had a second primary malignancy, and 8 (4%) of these additional malignancies were considered to have an estimated worse prognosis compared to the earlier diagnosed BC. In the whole population of 1337 patients, 1.3% had a second primary malignancy and 0.6% a more prognosis determining diagnosis than their current BC.
It is widely recognized that FDG-PET/CT frequently reveals incidental findings. The incidence of these findings depends on patient population and the definition of an incidental finding [14,15,16,17, 20]. Older patients and patients with malignancies tend to have a higher number of incidental findings on FDG-PET/CT [14]. Variations in the definition of incidental findings across studies is seen, as some studies report all additional findings, while others focus only on suspected incidental findings. The incidence rates in these reports range from 12–75%, in this study in 28% of the patients an additional finding was reported [14, 15]. The decision to further evaluate an incidental finding depends on patient-specific factors, the level of suspicion associated with the finding and the treating physician’s assessment. In a study conducted by Srour et al., it was reported that 146 out of 262 (55.7%) patients who underwent FDG-PET-CT prior to NAC had incidental findings [20]. This study included patients with findings deemed “likely” to be physiological, and no further work-up was outlined for these findings. Moreover, Vogsen et al. conducted a study involving 103 patients with high-risk primary BC undergoing FDG-PET/CT, resulting in 24 (23%) patients undergoing examinations for incidental findings [21]. In a separate prospective cohort of 225 patients with suspected recurrent BC undergoing FDG-PET/CT, Vogsen et al. observed incidental findings necessitating further examinations in 46 patients (20%) [22]. These results align with the 15% incidence observed our study. There is currently a lack of national or international guidelines addressing the management of additional findings on FDG-PET/CT scans.
To gain better insight on the current work-up of additional findings on FDG-PET/CT, we specifically focused on patients who had a non-BC-related finding that was deemed non-physiological and who underwent additional diagnostic work-up. In this group a high number of diagnostic work-up was performed (318 examination sin 202 patients), resulting in the detection of only 17 (17/202 = 8% or 17/1337 = 1.3%) new malignancies, which seems to align with previous literature. In two separate studies conducted by Beatty et al. and Hadad et al., cancer patients who underwent a FDG-PET/CT were found to have a second primary malignancy in 1.8% and 0.6% of cases, respectively [15, 16]. Vogsen et al. reported a second primary malignancy in 3.8% of high-risk BC patients undergoing FDG-PET/CT.[21]Notably, 10 patients in this study were diagnosed with thyroid cancer, which is a frequently reported incidental finding on FDG-PET/CT scans [23]. A correlation between BC and thyroid cancer has been reported; thyroid cancer occurs at an incidence of 0.1% among patients with BC [24]. In our study, we observed thyroid cancer in 0.74% of the patients, consistent with the existing literature. Most of these cases were papillary thyroid carcinomas (9/10, 90%), which has a favorable prognosis with a 10-years overall survival of 97% [25]. Therefore, we considered a papillary thyroid carcinoma not to be prognosis-determining.
In general, to minimize unnecessary work-up, nuclear medicine physicians consider various variables (such as BC stadium, localization of the incidental finding and the pattern of FDG uptake) to assess whether a lesion is suspected for a second primary malignancy or BC-related metastases. Advanced BC, high-FDG uptake in the primary tumor, focal aspect of FDG uptake, and high SUVmax and/or SUVpeak are associated with a higher likelihood of a (BC-related) malignancy. [17] Additionally, different sites necessitate different work-up strategies [17]. Nevertheless, our study reveals a persistently high rate of unnecessary diagnostic work-up procedures. During the second review of all FDG-PET/CT scans conducted by a nuclear physician, we found that 28% of our study patients who had undergone work-up for an initially reported non-BC-related additional finding, had no indication for further work-up in retrospect. In the group of additional endocrine findings, 9 out of 46 (20%) thyroid glands showed diffuse uptake. These lesions were not suspected by the second reviewer and none of these lesions turned out to be a malignancy. It is already known that these non-focal uptake sites are mostly physiological of benign and therefore not necessary to be pursued by additional work-up [26]. Furthermore, we discovered that 24 of the 31 initially reported lung nodules (77%) were non-specific millimetric lung nodules lacking FDG-uptake that, in hindsight, do not need further work-up. We suggest that all additional lung findings warrant a routine thorough scoring assessment using the Fleischner criteria to avoid unnecessary follow-up [27]. Additionally, we found that distant lymph nodes were investigated even in the absence of suspected axillary lymph nodes or the presence of an obvious infectious focus. In such cases, these lesions are more likely to be considered as physiological or benign. Similarly, in the case of FDG uptake in the urogenital region, which is often influenced by hormonal fluctuations, these lesions may also be more frequently regarded as physiological. However, caution is needed in patients with a BRCA genetic mutation or in patients of older age. Finally, diffuse uptake in gastrointestinal and liver lesions should also mostly be interpreted as unsuspected. It is recommended to explicitly report these findings as physiological or benign. By addressing these specific findings and highlighting their unsuspected nature, we can avoid unnecessary investigations and provide more accurate guidance for clinical decision-making.
It should be noted that FDG-PET/CT offers many advantages. In the regional setting, FDG-PET/CT demonstrates high sensitivity for detecting regional metastases, resulting in changes of locoregional treatment (i.e. surgery and/or radiotherapy) [10, 28, 29]. Furthermore, FDG-PET/CT is superior to conventional imaging in detecting distant metastases, influencing treatment decisions [11, 12]. In this study BC-related findings, i.e. metastases are excluded. In this cohort 112/1337 patients eventually had distant metastasis on FDG-PET/CT [11]. We found a low incidence of non-BC related additional findings in the bone, liver, and distant lymph nodes. However, since these organs are known to be preferred metastases sites, it is premature to conclude that additional findings in these locations do not necessitate further investigation in all cases [30].
This study has certain limitations that should be acknowledged. First, it was conducted at a single tertiary cancer center, which may limit the transferability of the findings to other hospitals. Furthermore, it is important to acknowledge that our study primarily relies on retrospectively gathered information extracted from FDG-PET/CT reports. For inclusion in the study, the patients needed to have an additional finding mentioned in the report followed by diagnostic work-up. It is important to note that these reports may be influenced by the subjectivity and variability of the reporting nuclear physician, as different physicians might interpret and report findings differently. Additionally, we cannot be certain whether the nuclear physician intended to advise diagnostic work-up solely by mentioning the finding in the FDG-PET/CT report, because often there was no level of suspicion reported. However, as a result of this, our study provides valuable insight into daily clinical practice. Furthermore, it is important to acknowledge the potential for slight bias in the revising nuclear physician’s evaluation, given that only the 202 FDG-PET/CT scans with additional non-BC-related additional findings were reviewed. While the revising nuclear physician was blinded for the initial reports and the final diagnosis, the selective review of scans could introduce a subtle bias. Additionally, considering inter-rater variability, the revising nuclear physician was very experienced, whereas the initial reports were authored by different nuclear physicians with varying levels of experience. This diversity in experience might have contributed to the variability in the interpretation of the non-BC-related findings across the FDG-PET/CT scans.
In conclusion, this study underscores the high rate of additional invasive diagnostic examinations performed for non-BC-related FDG-PET/CT findings, resulting in only a limited number of clinically relevant findings. In case of performing FDG-PET/CT it is important to balance out the advantages of improved staging and early detection of secondary primary malignancies in 1.3% of patients with the disadvantages of invasive work-up for irrelevant non-BC-related findings, challenging logistics and costs. Besides further specifying the need for FDG-PET/CT in patients with BC eligible for NAC, physicians must be aware of the low-clinical relevance of non-BC-related additional findings. Still, it must be kept in mind that there is a slight change of early detection of a second primary malignancies with good treatment options. We recommend a multidisciplinary approach to determine the need for further work-up of all FDG-PET/CT additional lesions and to limit the amount of invasive procedures with an expected low yield for relevant findings. Future studies about cost-effectiveness of FDG-PET/CT in patients with BC eligible for NAC or the implementation of artificial intelligence to determine which non-BC-related findings need diagnostic work-up would ideally lead to an unambiguous guideline.


留言 (0)