Characteristics and participants of the selected clinical trial
A prospective, double-blind, randomized controlled trial of central retinal artery occlusion (trial ID in the Japan Registry of Clinical Trials: jRCT2021190013) was selected to evaluate the R2BM methodology. The study duration for each participant was 12 weeks and included 6 visits: weeks 0, 1, 2, 4, 8, and 12. Twenty participants were randomized and administered the study treatment. R2BM was conducted with only the last 8 of the 20 participants because the present study started in the middle of the selected clinical trial. On-site monitoring reviewing all records in the source documents of the 20 participants was conducted within 4 weeks after weeks 4 and 12 for each participant by on-site monitoring clinical research associates (on-site CRAs). EDC was used for data collection, and data entered into the EDC were reviewed on time by a data manager (DM) without confirming any source document.
Remote monitoring system
A remote monitoring system called beagle View®, developed by beagle Co. Ltd., was used for R2BM. The system is a cloud-based application downloaded to a tablet device prepared exclusively for this study that enables remote monitoring through the following steps: (1) clinical trial staff capture photographs of source documents, such as EHR screens and paper worksheets, using the device’s camera; (2) clinical trial staff upload the photographs immediately to a folder designated for each participant’s visit to a secure cloud location by selecting several photographs saved on the tablet device without any additional procedure such as changing the file name; and (3) a remote monitoring CRA (remote CRA), different from on-site CRAs, views the photographs remotely in a private room.
Personal information was included in the uploaded photographs without masking. Therefore, appropriate written informed consent was obtained from all participants for handling personal information. In addition, all researchers received training on procedures to protect the participants’ personal information.
R2BM plan
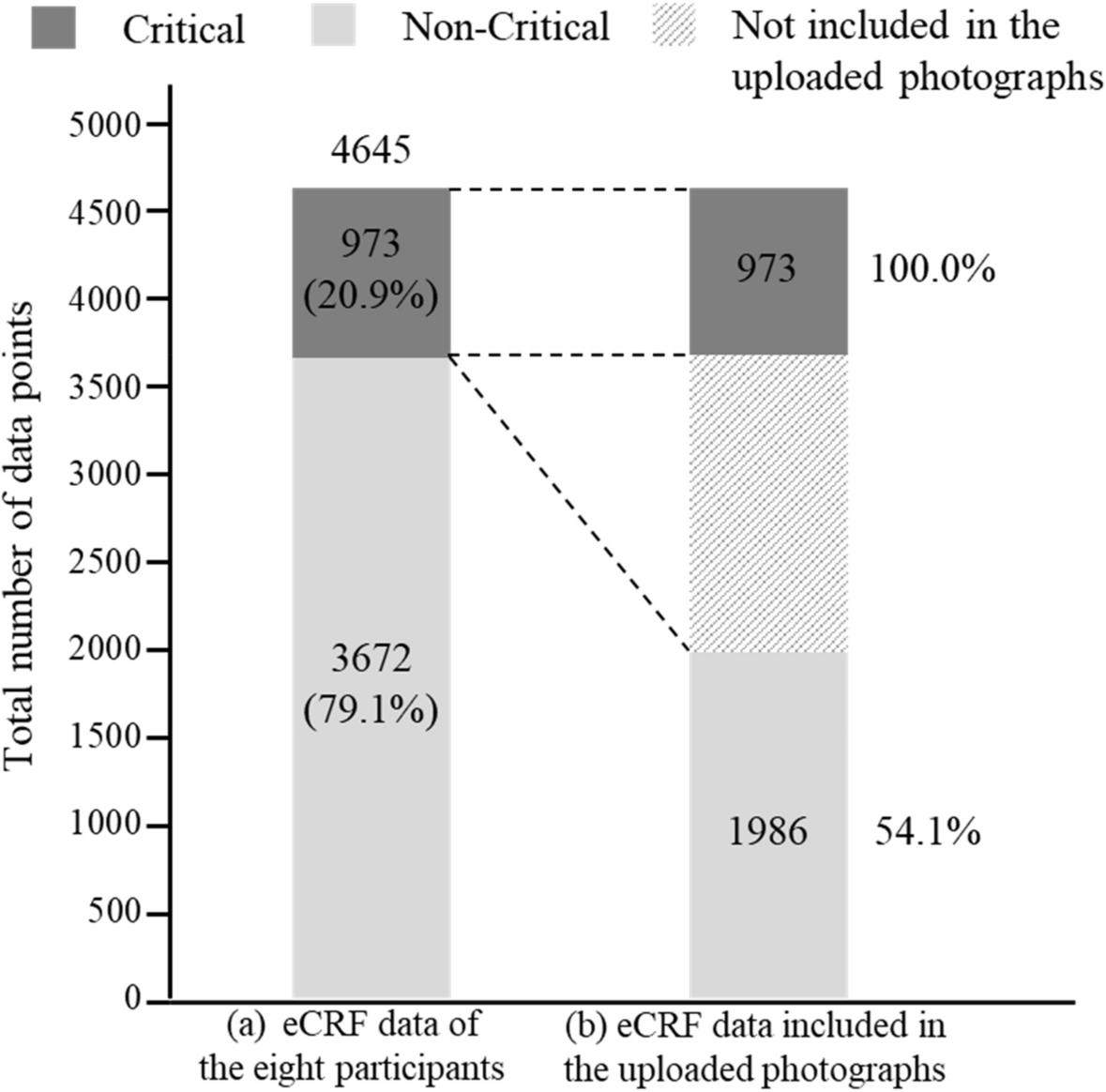
Data and processes related to the following items were defined as critical: (1) informed consent, (2) eligibility criteria, (3) visit date, (4) randomization, (5) study treatments, (6) primary endpoint, (7) treatment compliance, (8) stratification factors for the primary endpoint, (9) adverse events, and (10) discontinuation. The risks that could lead to critical process errors were identified by referring to the risk assessment and categorization tool developed by TransCelerate BioPharma Inc. [18].
To ensure the capture of photographs of source documents that the remote CRA needed to review, a source document identification list defining when and which source documents should be captured and uploaded was created by discussing with the clinical trial staff. Only the source documents necessary to confirm 100% of the critical data, critical processes, and identified risks were included in the list.
The R2BM plan required the clinical trial staff to capture and upload only photographs of the source documents defined in the list within 2 weeks after weeks 0, 1, 2, 4, and 12 for each participant. The photographs from week 8 were captured and uploaded simultaneously with those from week 12.
The remote CRA verified only critical data (targeted SDV) and reviewed only critical processes (targeted source data review; targeted SDR) without delay after uploading the photographs. If the remote CRA found the photograph inappropriate or missing, the clinical trial staff were asked to re-capture and upload the photographs.
Implementation of R2BM
The remote CRA independently performed R2BM on the same eight participants in parallel with on-site monitoring by the on-site CRAs and data review by the DM. No data and process errors were shared between the remote CRA and the on-site CRAs or the DM.
After completing the R2BM, the remote CRA visited the clinical trial site and confirmed all data, processes, and source documents to evaluate the ability of R2BM to detect data and process errors and the accuracy of the uploaded photographs.
Evaluation of R2BM methodologyEvaluation of the ability of R2BM to detect data and process errors
Data errors were defined as eCRF data corrected at least once. Process errors were defined as source records determined or else suspected to be protocol deviations. Because on-site monitoring, R2BM, and data review by DM were conducted independently and in parallel, we considered whether data and process errors detected by each method were also theoretically detectable by other methods based on the definitions in Table 1 and tallied.
Table 1 Definitions of data errors theoretically detectable by each methodEvaluation of the additional workload of R2BM for clinical trial staff
We measured the time to capture and upload photographs in units of 5 min and counted the number of uploaded photographs. Fractional minutes were rounded up to the closest 5-min unit.
Evaluation of uploaded photograph accuracy
Because R2BM was conducted based on information included in uploaded photographs, it was necessary to evaluate their accuracy. After completing the R2BM, the remote CRA visited the clinical trial site and confirmed all source documents. These documents were compared with those uploaded to the cloud, and the number of inappropriate photographs was counted and classified into the categories shown in Table 2.
Table 2 Definitions of photographs judged as inappropriate by the remote clinical research associateEvaluation of the period from each participant’s visit to photograph upload
Because clinical trial monitoring should be conducted in a timely manner following the monitoring plan, uploading photographs within 2 weeks after each participant’s visit was defined in the R2BM plan. To evaluate compliance with that requirement, the number of times to upload and the number of days from each participant’s visit to the upload of photographs were determined.
Evaluation of the synergistic effects of DDC on R2BM methodology
By entering clinical trial data directly into eCRF, DDC can minimize the transcription of clinical trial data from source documents to the eCRF and reduce the number of data points requiring SDV. This may have reduced the number of photographs of source documents captured for R2BM. The following evaluations were conducted to clarify this benefit, assuming DDC was introduced for data collection instead of EDC in this study.
Evaluation of the number of data points that can be entered directly into eCRFs without transcriptions by introducing DDC
Not all data can be entered directly into the eCRFs without transcriptions, even though DDC is used for data collection because data generated in daily medical practice are recorded in the EHRs as source data. To evaluate how much data would be entered directly into the eCRFs without transcriptions by introducing DDC, the eCRF data were classified into category I (data not requiring transcriptions and SDV by introducing DDC) or category II (data requiring transcriptions and SDV despite introducing DDC) by discussing with the clinical trial staff and then counting. Detailed definitions of the categories are illustrated in Table 3.
Table 3 Definitions of data points classified as category I or category IIEvaluation of the proportion of data errors detectable only by SDV despite introducing DDC
Errors in the data classified as category I would not occur or could be detected by data review because the data can be entered directly into the eCRFs without transcriptions by introducing DDC. Although data classified as category II require SDV, errors in these data can be further classified into errors detectable by data review (category II-A) or only by SDV (category II-B). To evaluate how many data errors were detectable only by SDV when DDC was introduced (category II-B), the eCRF data errors were classified into one of the categories and counted.
Evaluation of the workload of R2BM reduced by introducing DDC
When DDC was introduced for data collection, data classified as category II would still require transcriptions and SDV. In the R2BM methodology focusing only on critical data, the clinical trial staff are only required to capture photographs of source documents, including critical data classified as category II. To evaluate how much the workload of R2BM was reduced by introducing DDC, the proportion of photographs not including critical data classified as category II was determined.
Statistical analysis
Data points, the proportion of data errors, the accuracy of uploaded photographs, and the workload of R2BM that could be reduced by introducing DDC were calculated as proportions and presented as percentages and frequencies with 95% confidence intervals (CI) [19]. The number of uploaded photographs and the time to capture and upload photographs is expressed as mean ± standard deviation (SD). The number of days from each participant’s visit to the upload of photographs is shown as the median and interquartile range (IQR).






留言 (0)