
記住我








The comparator (placebo) has been chosen because there are currently no approved medications for methamphetamine use disorder.
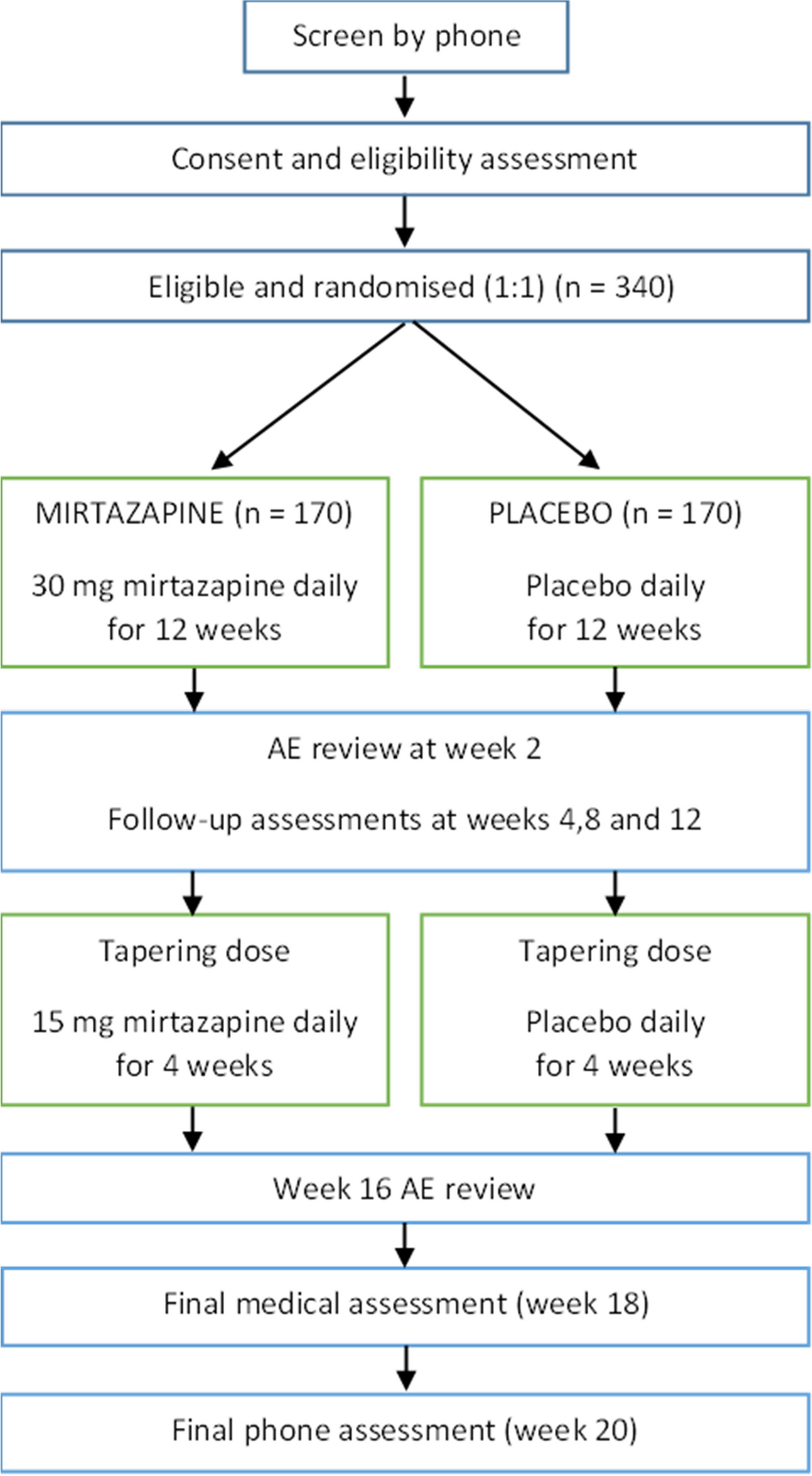
Intervention descriptionThe intervention is daily oral mirtazapine 30 mg per day, or matched placebo, for 12 weeks, taken as one tablet each evening. This is provided in bottles of 35 tablets at baseline, week 4 and week 8. A tapering dose of 15 mg per day, for 28 days, is provided at week 12. All participants are provided with a self-help booklet (“On Ice”, National Drug and Alcohol Research Centre, University of New South Wales), referral information for local health services, and have access to usual care during the study.
Criteria for discontinuing or modifying allocated interventionsThe participants are free to discontinue the trial medication at any time. The trial medication may be temporarily discontinued by the study team (e.g., to monitor an adverse event or suspected pregnancy). The study team may permanently discontinue a participant from the trial medication if they become pregnant, develop contraindications for mirtazapine, are diagnosed with a medical condition that significantly increases their risk of AEs, or are unable to comply with the study protocol to an extent that significantly compromises their safety (e.g., unable to attend medical assessments). Participants may be temporarily or permanently changed to a 15-mg dose of the trial medication in response to adverse reactions to the trial medication. Participants who are discontinued from the medication remain in the study to complete study assessments (unless they are also withdrawn from the study or withdraw their consent to participate).
Participants are free to withdraw from the study at any time. The study team may withdraw participants from the study if:
The participant is unable to complete study procedures (e.g., becomes incarcerated),
There is significant non-compliance with the study protocol and/or behaviour that compromises the safety and wellbeing of the trial participant or the trial personnel, or
If the participant meets an exclusion criterion that precludes further study participation.
If a participant withdraws from the study, or is withdrawn by the study team, they are not followed up for further assessments. However, they will be asked to attend a final medical assessment to review AEs and to return their study medication.
Strategies to improve adherence to interventionsAdherence to the trial medication (baseline to week 12) is monitored using a medication event monitoring system, MEMS® Smart Caps, which record the time and date of each bottle opening. Adherence data is reviewed at week 4 and week 8, and participants are counselled on adherence strategies. An adherent dose is defined as any bottle opening in a 24-h period (ending at 3 am) with no penalty for multiple openings. MEMS® Smart Caps® also display the number of bottle openings each day so that participants can see when they have taken their daily dose.
Relevant concomitant care permitted or prohibited during the trialParticipants may engage in treatment as usual throughout the trial. Where this precludes participation in the trial (either for logistical or safety reasons) participants may be discontinued from the trial medication or withdrawn from the study.
Provisions for post-trial careAt the end of the trial, all participants are offered a referral to substance use treatment, including a referral for the ongoing prescription of mirtazapine. Participants who suffer harm from trial participation can seek compensation in accordance with the Medicines Australia Compensation Guidelines (https://medicinesaustralia.com.au/policy/clinical-trials/indemity-and-compensation-guidelines/).
Outcomes Primary outcomeReported days of methamphetamine use: The primary outcome is a change in self-reported days of methamphetamine use in the past 4 weeks from baseline to week 12. Self-reported days of methamphetamine use are assessed using the Timeline Followback (TLFB) [19]. The TLFB is a retrospective self-report measure that uses a calendar to aid recall. It has 88% sensitivity and 96% specificity against amphetamine urine test results, and 0.77 test–retest agreement [20]. TLFB data will be validated against biologically verified abstinence from methamphetamine use.
Secondary outcomesAbstinence from methamphetamine use: Methamphetamine-negative oral fluid samples (< 25 ng/mL methamphetamine) taken at weeks 4, 8 and 12 using a commercial oral fluid collection device. Oral fluid is a sensitive and stable medium for the detection of methamphetamine and correlates highly with plasma tests [21].
Depressive symptoms: Total score on the Patient Health Questionnaire-9 (PHQ-9) [22] at week 12. The PHQ-9 is a brief 9-item questionnaire that has excellent internal consistency (Cronbach’s alpha of 0.89), test–retest reliability (r = 0.84) and good construct validity against other measures [22].
Sleep quality: Total score on the Athens Insomnia Scale (AIS) [23] at week 12. The AIS is an 8-item self-report measure which has 0.9 test–retest reliability and has been validated against other measures of sleep quality [23].
HIV risk behaviour: Total score on a modified version of the HIV Risk-taking Behaviour Scale (HRBS) from the Opioid Treatment Index [24] at week 12. The HRBS is a validated and reliable scale that provides a composite risk index for injecting and sexual behaviour. The modified version of this scale is available from the authors on request.
Quality of life: The utility score on the EuroQol-5D-5L (EQ-5D) [25] at week 12 is used to measure quality of life.
Tertiary/exploratory outcomesSuicidality: Scores of 3 or greater on the Columbia Suicide Severity Rating Scale Screener (CSSRS-S) [26, 27] at any time in the 12-week active medication phase. A score of 3 or more on the CSSRS-S predicts a significant increase in the risk of a subsequent suicide attempt [27].
Other substance use: Total days of use for other drug classes (tobacco, alcohol, cannabis, cocaine, ecstasy, hallucinogens, inhalants, and heroin) in the 4 weeks prior to the week 12 assessment.
Treatment satisfaction: Scores on the Treatment Satisfaction Questionnaire for Medication Version II (TSQM II) [28] at week 12 are being used to assess treatment satisfaction. The TSQM II provides a global satisfaction summary score and subscale scores for medication convenience, side effects, and effectiveness. Additional questions have been included at other weeks to assess tolerability and expected reactions to mirtazapine.
Anxiety: Total scores on the Generalized Anxiety Disorder – 7 Item (GAD-7) [29] at week 12. The GAD-7 is a validated screening tool for generalised anxiety disorder that can also be used to assess the severity of anxiety [29].
Participants’ impression of their health status: The score on the single-item Patient Global Impression – Improvement (PGI—I) [30] is used at week 12 to assess whether participants perceive that their health status has improved since the start of the trial.
Concomitant medications: All medications taken by participants during the trial are recorded on a template adapted from the National Institute of Health Concomitant Medications Form [31].
Health economics: Health economics data collected include the EuroQol 5D [25] and the Work Productivity and Activity Impairment Questionnaire – General Health (WPAIQ-GH) V2 [32] at week 12, and contact with health services and the criminal justice system from baseline to the week 12 assessment.
Adverse events (AEs): The percentage of participants reporting AEs, and serious adverse events (SAEs), by System Organ Classification, will be coded according to the Medical Dictionary for Regulatory Activities (MedDRA) [33]. AEs will be counted once only for a given participant.
Participant timelineAll participants undergo an initial phone screening and eligibility assessment, after which they have evaluation assessments at baseline, week 4, week 8, week 12, and week 20. They also have an initial medical screening (as part of the eligibility assessment), a final medical review (week 18), and two additional phone follow-ups to review AEs at weeks 2 and 16. The detailed schedule for assessments is provided in Table 1, and the study flow chart is presented in Fig. 1.
Table 1 Schedule of enrolment, interventions and assessmentsFig. 1
Flow diagram for the trial
Sample sizeThe sample size (N = 340; 170 per group) will enable us to detect a minimum rate ratio of 0.75 on our primary outcome (equivalent to a reduction from 25 days of methamphetamine use in the past 4 weeks at baseline to 20 days of use in the past 4 weeks at week 12) with 90% power (two-tailed test, p = 0.05). This sample size calculation is based on the effect size found in the most recent trial of mirtazapine for methamphetamine dependence [15] and allows for up to 25% attrition.
RecruitmentParticipants are being recruited from the community via advertisements (e.g., local newspapers, free press, and social media), flyers (e.g., placed in needle and syringe programmes, community health care centres) and word of mouth. Participants can also be referred from helplines, health services, and other research studies.
留言 (0)