This study describes uUTI treatment in a large female population in Germany. Most patients received antibiotic treatment that was non-concordant with German treatment guidelines. Compared with the non-recommended treatment sub-cohort, patients who received recommended treatment tended to be younger and have less impact of comorbidities. Adherence to treatment guidelines varied by physician specialty. GPs were markedly more likely to prescribe a treatment that was non-concordant with the guidelines compared with specialist physicians.
Most patients (85%) had optimal outcomes, defined by the absence of additional antibiotic prescriptions and no indication of a worsening of uUTI. Interestingly, we observed among patients who had optimal outcomes, a higher proportion received antibiotics recommended but not as first-choice (59%) for the initial uUTI episode compared with first-choice therapies (35%); this pattern was observed to a lesser extent in the sub-optimal outcome cohort (49% received recommended but not as first-choice therapies, 41% received first-choice therapies). This unexpected result may speak to the challenges of empirical prescribing in the context of rising antimicrobial resistance in the community.
Antibiotic Prescribing Patterns
Overall, the most frequently prescribed antibiotic for initial uUTI treatment was fosfomycin (30.4%), which is recommended for first-choice therapy per German clinical practice guidelines, followed by ciprofloxacin (27.0%) and sulfamethoxazole/trimethoprim (19.9%). Sulfamethoxazole/trimethoprim and ciprofloxacin treatment are not recommended for first-choice uUTI therapy in Germany but are still recommended [11]. However, despite the guidance provided, a recent survey highlighted fosfomycin and sulfamethoxazole/trimethoprim as the preferred first-choice treatment choices among German physicians, chosen by 61% and 50% of 100 respondents, respectively [13]. Ciprofloxacin was the most commonly selected option following treatment failure (45%) [13]. In the current study, ciprofloxacin was the second most frequently prescribed antibiotic for first-choice treatment, with fluoroquinolone-class therapies accounting for 37% of all antibiotic prescriptions. An analysis of German health insurance data from 2015 to 2019 demonstrated movement towards more guideline-adherent prescribing practices, but with room for improvement regarding the use of antibiotics not recommended as first-choice therapies [14]. The discussion on the relevance of the recommended first-line drugs when second-line antibiotics are more effective is the dilemma for any guideline committee; ciprofloxacin (or other fluoroquinolones) are known to be effective for UTI [15], but they are also most prone to resistance [14]. However, if the diagnosis of UTI is not often validated and therefore treatment not administered for an actual infection, it may be preferable to use a less resistance-prone antibiotic for empiric first-line treatment. The resistance levels in Germany in E. coli for fluoroquinolones and sulfamethoxazole/trimethoprim points in the direction, that they should not be recommended as first-line empiric treatment [15].
Physician Specialty
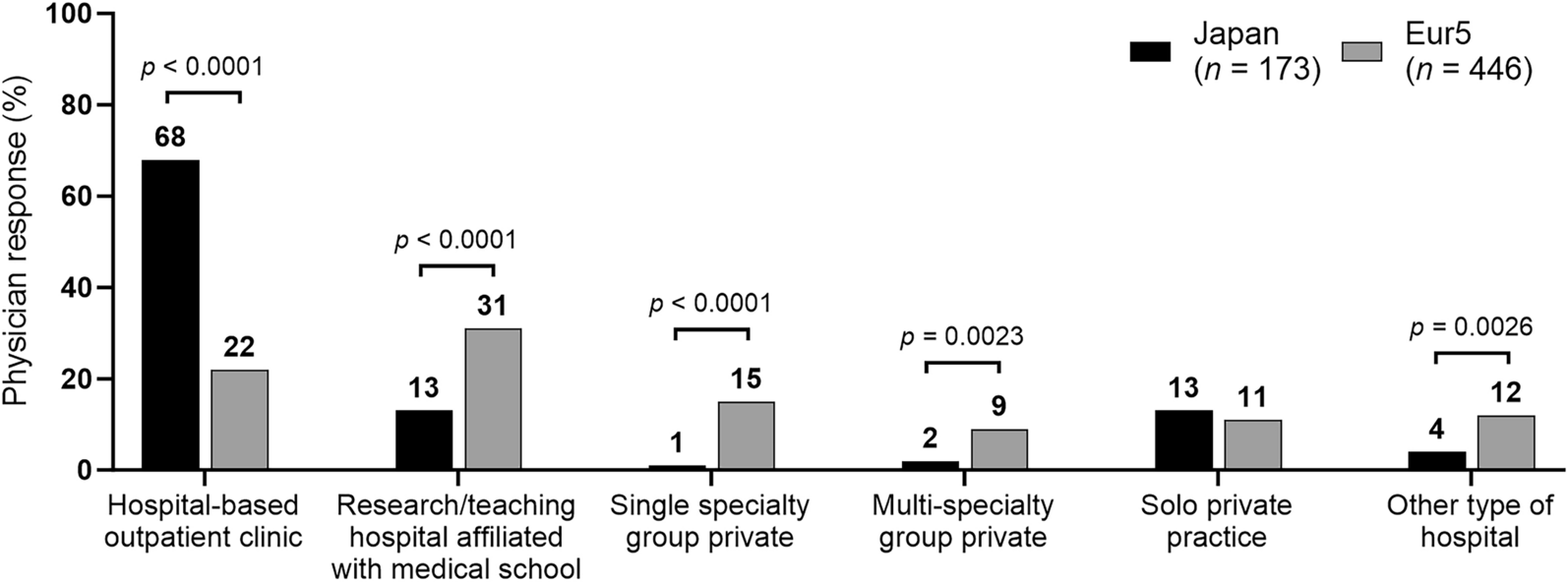
Most uUTI cases were diagnosed by GPs (fewer cases were diagnosed by gynecologists and urologists), and 64.6% of cases were treated with non-recommended initial therapies. GPs prescribed first-choice antibiotics in just 32% of cases and were found to provide non-recommended treatment to 68% of cases overall. Conversely, gynecologists prescribed mostly first-choice antibiotics and complied with guidelines in 60% of cases. High rates of non-recommended antibiotic prescribing are not unexpected, and they are not limited to Germany. Retrospective database studies of female patients with uUTI in the US have shown similar trends of guideline non-compliant antibiotic prescribing [16, 17]. One such study demonstrated a 45% rate of fluoroquinolone prescribing as first-choice, which fell by just 3% after guidelines were released, indicating a minimal impact of clinical guidance on prescribing behaviors [16]. High rates of guideline non-compliant antibiotic prescribing may contribute to antimicrobial resistance and potentially sub-optimal patient care [15, 18,19,20].
The outcome of the index episode was optimal in approximately 85% of cases, with comparable rates of optimal outcomes between the recommended treatment and non-recommended treatment cohorts (83% vs. 86%, respectively). Considering the high number of recommended prescriptions from gynecologists, this finding may be a result of complicating factors treated by specialists rather than GPs.
Limitations
This study was not without its limitations. First, given that empiric therapy was recommended by the German guidelines, it is possible that in some cases cultures were performed before therapy and the results of the cultures would impact the choice of therapy. These cases would differ from those experienced by the overall uUTI population, and the decision to deviate from the guidelines was not documented. However, while prescriptions were not directly linked to a diagnosis, it could be linked to the diagnosing physician by matching the unique ID of a physician involved in outpatient care to the ID of the physician who prescribed the antibiotics. In addition, one study found that the use of urine culture and susceptibility testing for guiding initial therapy for uUTI differed depending on physician and was more commonly used for initial therapy in the US (33–78%) versus Germany (9–50%) [13]. It is therefore likely that not all diagnoses were based on cultures. Another study found that symptoms of UTI do not necessarily equate to a culture-based UTI diagnosis [21]. Furthermore, it may be that, among the 85% of people who responded to antibiotic treatment, some may have had a false-positive UTI diagnosis. Similarly, sub-optimal outcome was defined as a switch in medication or documented ED or inpatient visit. As clinical and laboratory data were not available, the correlation of culture results with a switch in therapy could not be confirmed and non-recommended therapy may have been overestimated. Treatment with antibiotics not recommended as first-choice therapy could not be differentiated due to lacking information on antibiotic allergy and intolerance; this information could justify the use of an antibiotic not recommended as first-choice therapy in cases with limited treatment options.
On the other hand, services and prescriptions are documented with an exact date, the latter with a date of prescription and dispensing; however, prescriptions are not directly linked to a diagnosis, but by matching the unique ID of a physician involved in a case of outpatient care to the ID of the physician who prescribed the antibiotic. This could have led to misclassification if other infections requiring antibiotic treatment were diagnosed by the same physician. To avoid this misclassification, cases with other acute infections were excluded. Requiring linkage of diagnosis and prescription enabled the date of uUTI diagnosis, and thus the index date, to be extracted. It was presumed that any prescription was paralleled by a diagnosis, and cases with prescriptions that lacked an associated diagnosis were ignored.
It is also important to consider the limitations inherent to observational retrospective studies using claims data. Claims data can only demonstrate association and not causality, and the data described in this study were collected for the purpose of payment, not research. In addition, there was no precise method of identifying patients with uUTI using statutory health insurance claims data. Therefore, the epidemiological parameters were approximated by selecting adolescent and adult female patients with UTI diagnoses compatible with uUTI and excluding patients with indications of cUTI. The presence of a diagnosis code on a medical claim was also not positive proof of disease, as the diagnosis code may be incorrectly coded or imprecise. Information on outcomes such as treatment failure were not available and claims for filled prescriptions did not indicate whether the medication was taken as prescribed. Dates for diagnoses are not available in German claims data, which prevented the evaluation of treatment and outcomes over time and led to the exclusion of more cases than necessary (due to an inability to exclude in a temporally precise manner). The records used will have underestimated the true number of outpatient visits and the number of cases with progression; these cases were likely excluded as unrelated infections. The exclusion of unrelated infections was necessary, however, as it minimized the potential for misclassification of other infections diagnosed by the same physician and facilitated extraction of the index date for each patient.



留言 (0)